
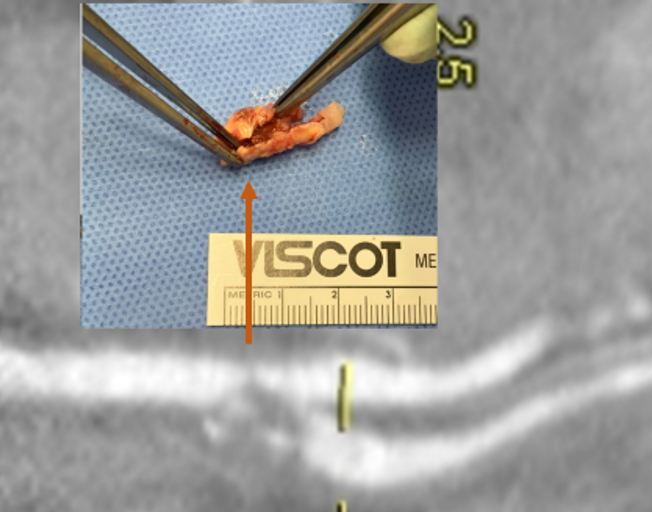
The patient is a middle aged executive who complains of bouts of aphasia triggered by intense conversations and business meetings. It first occurred while driving to Dubai on a conference call. Since then, they occurred several times a week, typically triggered during meetings where he needs to think and speak. Casual conversation and cognition does not seem to trigger this. Workup revealed a heterogeneous plaque affecting the left ICA with velocities in the 60-79% range. CTA confirmed this plaque. MRI failed to show any stroke or other lesions. Neurology evaluation showed normal exam. The patient underwent endarterectomy, and had a normal recovery. In followup, he denied any further episodes of aphasia.
Aphasia, the loss of function in the language centers, typically of the left brain, although in a minority, it may live in the right hemisphere, is terrifying manifestation of stroke. This case, if examined superficially, is nothing special in that TIA’s associated with a reasonable culprit lesion went away after elimination of that culprit lesion. To me, it was fascinating because it represents a possible case of brain claudication.
The human brain is believed to have evolved to its large size in conjunction with bipedalism, social hunting and gathering, and climate change in the Great Rift Valley favoring a savannah over forests, that created heat stresses on the brain, favoring the development of sweating and redundancies in brain tissue. The advent of fire and cooking enhanced available calories to feed this enlarged brain’s metabolic needs. When the metabolism isn’t supported through adequate blood supply, the brain tissue dies. Rarely, it blinkers on and off, and even more rarely, this occurs in the motor strip triggering today a neurologic evaluation including a carotid duplex that brings these patients to our attention. The fascinating question for me is, does increased metabolic demand in the form of complex thinking result in a supply-demand mismatch much as seen in exercise induced angina or claudication? If it can, can we test for it?
The tests we have available are hemodynamically based. At its simplest, after carotid angiography, an occluding balloon can be inflated to test for symptoms. This is an archaic test and I do not do it. There are nuclear medicine, PET CT, and MRI tests that use pharmacologic agents to induce hypotension, but again, for this patient, it wouldn’t apply. This patient needed the equivalent of a treadmill in the MRI machine. Maybe having him read a dry, technical treatise on neurobiology taped to the MRI tube?
I went to the OR with the indication of TIAs associated with a >50% lesion, but I did tell the patient that it was possible his thinking-induced aphasia would not remit. Thankfully it did.
