The dictum that better is the enemy of good is one of the old chestnuts carried around surgery training forever. It is an admonition against an unhealthy perfectionism that arises from either vanity or self doubt, and in the worse cases, both. The typical scenario is a surgeon trying to make a textbook picture perfect result and finding the patient’s tissues lacking, will take down their work to make it better, and repeat this process while the patient and everyone else in the room lingers.
Trying to avoid this, many surgeons will try to avoid any difficulties -the bad patch of scar tissue, irradiated body parts, areas of prior infection. But the mental contortions involved in avoiding “perfect” can result in actual physical contortions that in the end don’t pay off in good enough. I have not been immune to this, and I don’t think any physician or surgeon can honestly say they haven’t experienced some variation on this.
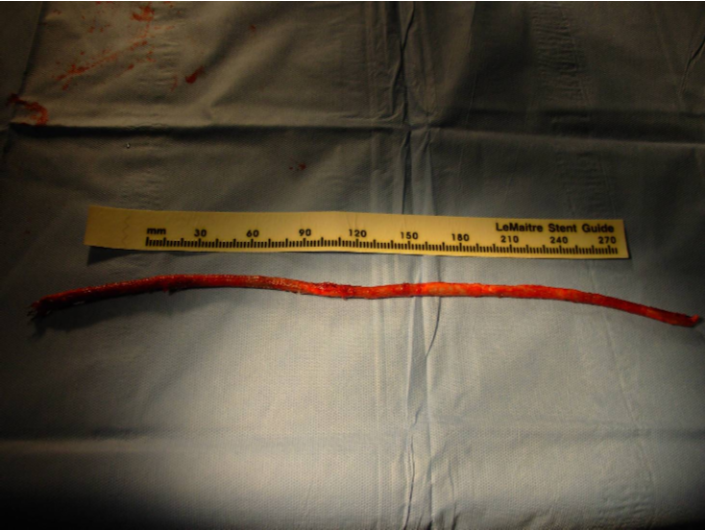
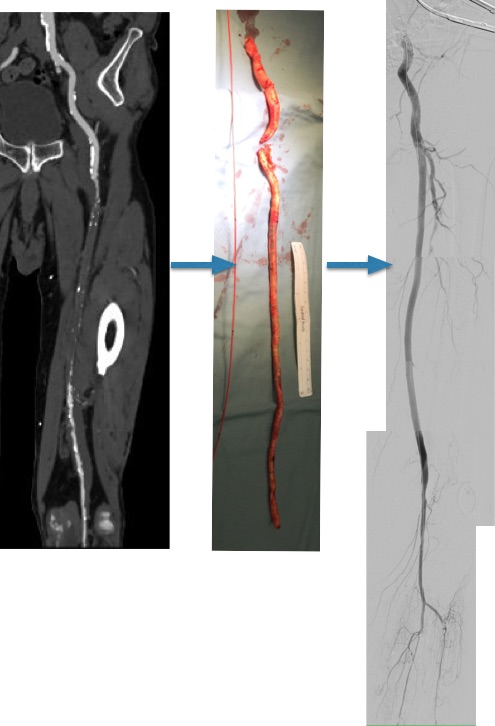
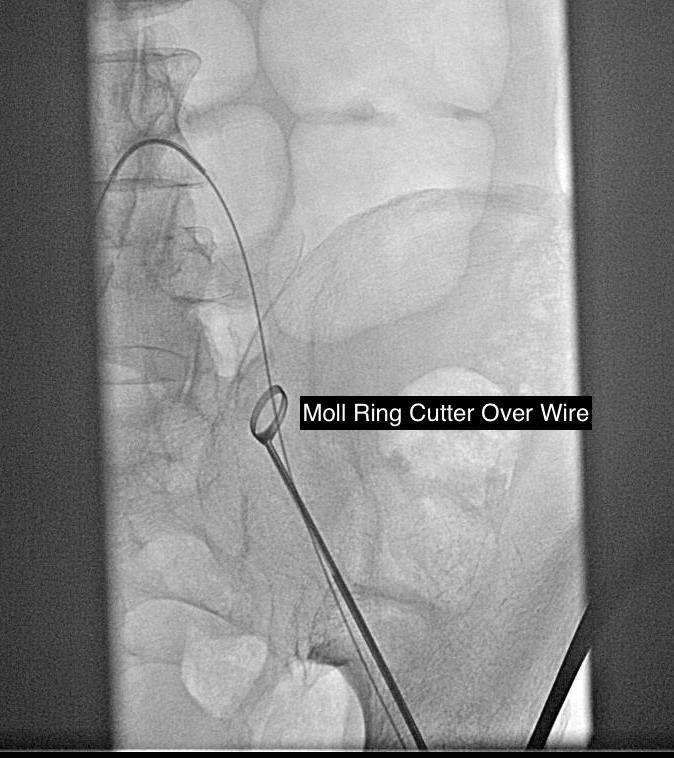
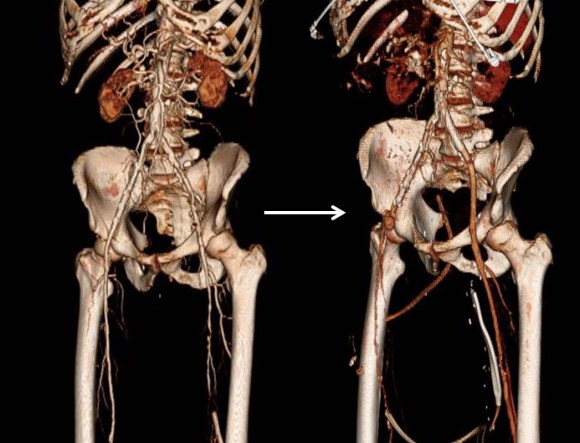
This patient is a younger middle aged man who in his youth experienced a posterior dislocation of his left knee, resulting in an arterial transection. This was repaired with an in-situ graft. Subsequently, he had complications of osteomyelitis and had his knee fused after resection of his joint. He did well with this bypass for several decades, but it finally failed several years ago, and a new one was created (image above).
Rather than directing the graft in line as in the previous one, this was was taken from a medial exposure of the femoral artery and tunneled superficially around the fused knee to coil lateral, ending in the anterior tibial artery.
This graft in turn thrombosed and was lysed by the outside surgeons and underwent serial interventions of proximal and distal stenoses at the anastomoses. The patient, when I met him, was contemplating an above knee amputation as a path to returning to work as a nurse in a rural hospital.
While there should be no reason long bypasses should do any less better than short bypasses, I do have to say these things about this patient’s bypass:
- No vein is perfect and the longer your bypass, the more chances you will have that a segment of bad vein will end up in your bypass
- Turning flow sharply can cause harsh turbulence. Turbulence can cause transition of potential energy into kinetic energy which acts to damage intimal, resulting in intimal hyperplasia.
- Thrombosis is a sure sign that your graft is disadvantaged, and the longer the period of thrombosis, the longer the intima “cooks” in the inflammatory response that accompanies thrombosis, making the vein graft even more vulnerable to subsequent intimal hyperplasia, thrombosis, or stricture.
- A high flow, small diameter vein graft entering a larger, disease free bed results in more turbulence but also Bernoulli effects that cause the graft to close intermittently, vibrating like one of those party favors that make a Bronx Cheer (a Heimlich valve). This is the cause I think of the distal long segment narrowing on this graft.
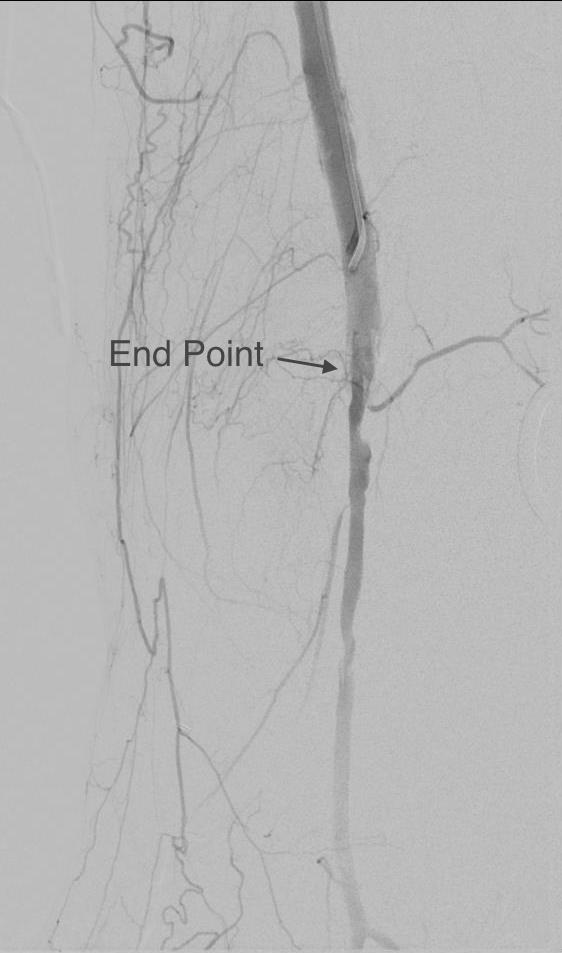
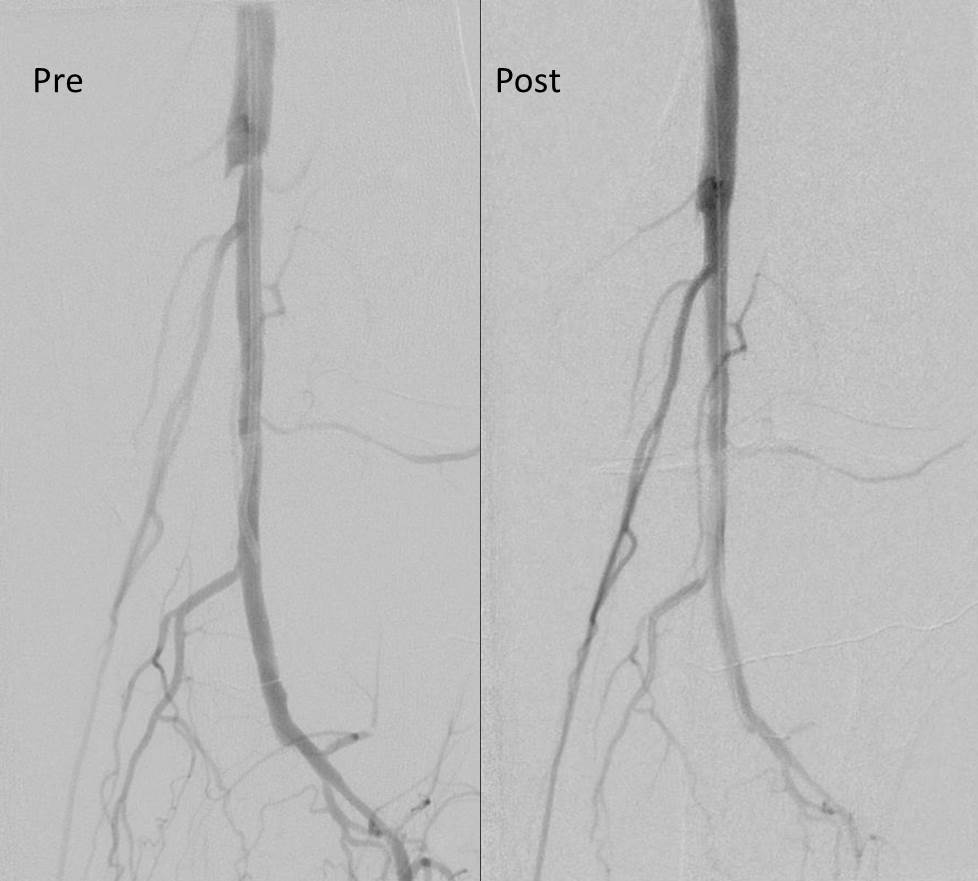
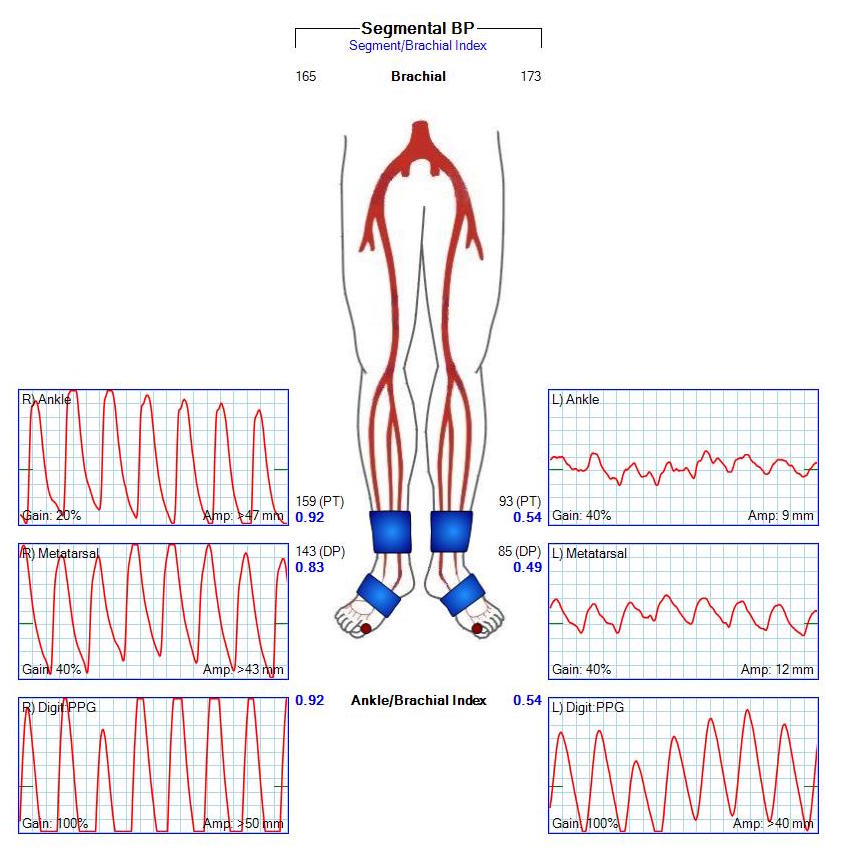
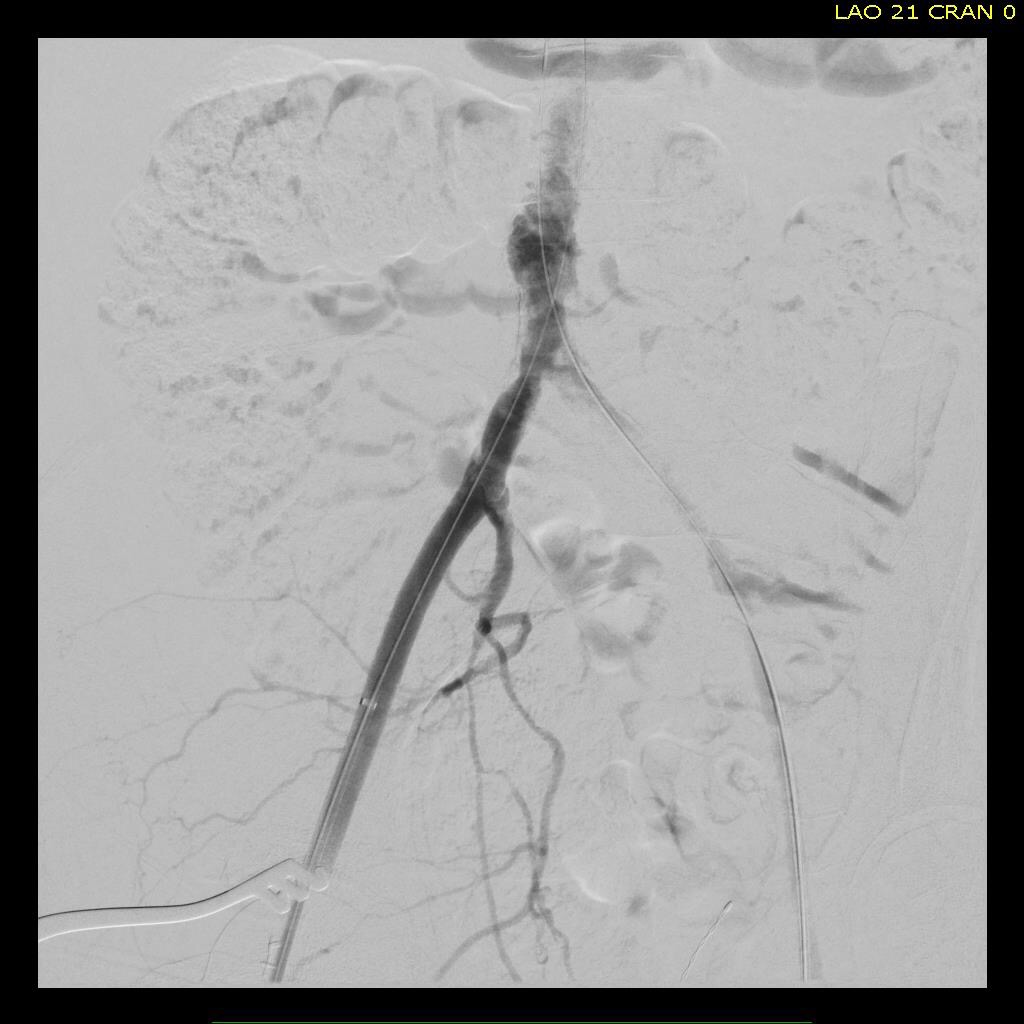
This patient was decided on amputation when our service was consulted, and after reviewing his CTA, I offered balloon angioplasty as his symptoms were primarily of paresthesia and neuropathic pain. I used cutting balloons and got angiographically satisfactory results.

The patient, although he admitted to feeling much better, was sad. He relayed that he had felt this way several times before, only to have his life interrupted by pain and weakness signaling a restenosis.

It was only a month later when I heard the patient had returned with the same symptoms. He wasn’t angry nor full of any “I told you so” that frankly I was muttering to myself. Reviewing his CTA, he had restenosed to a pinhole. The vein, to use a scientific term, was “no good.”
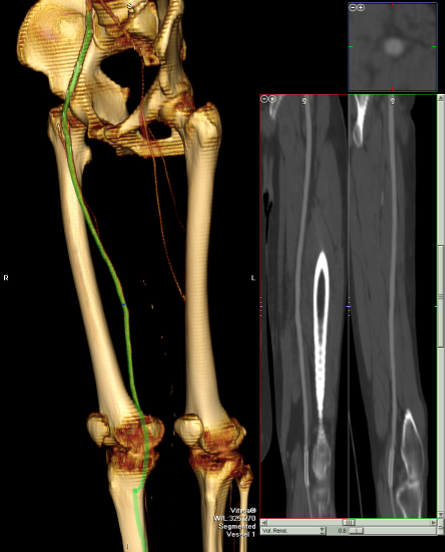
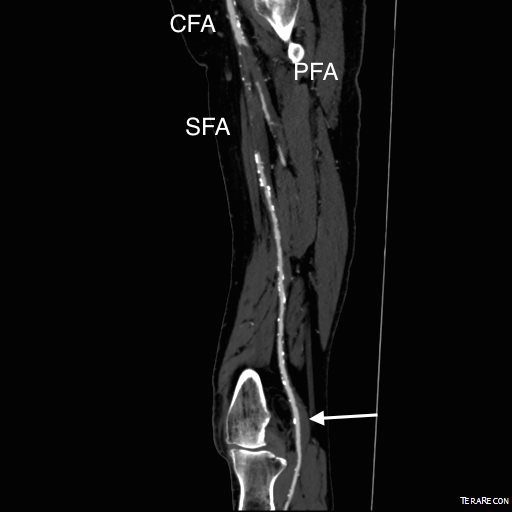
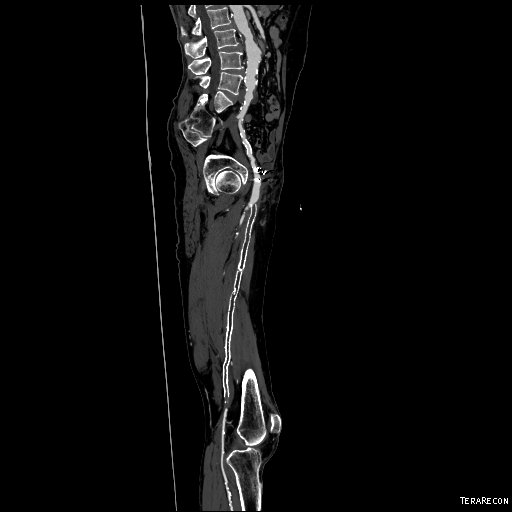
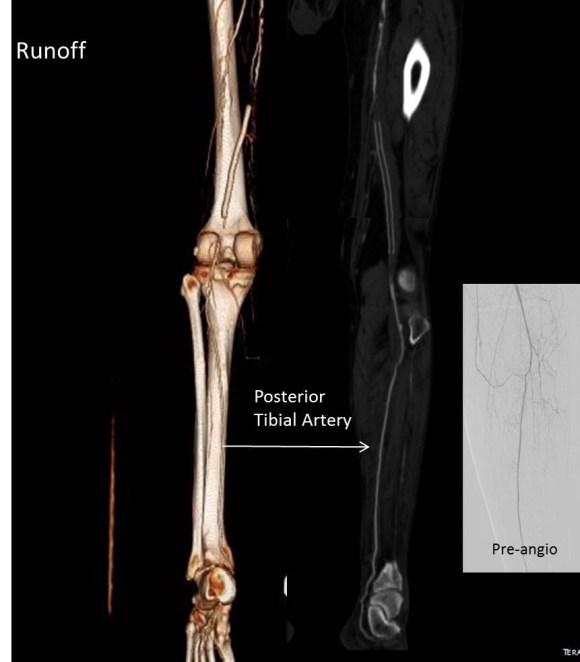
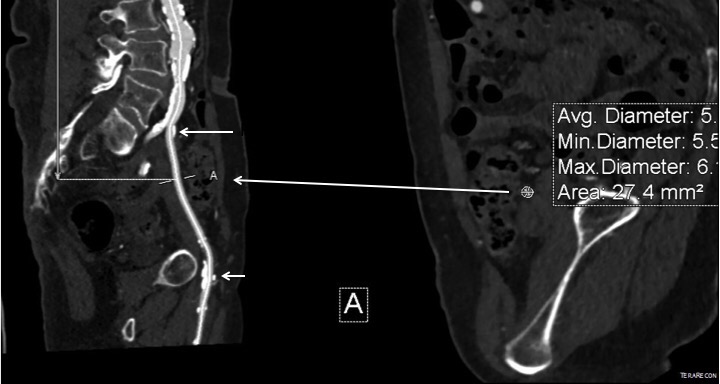
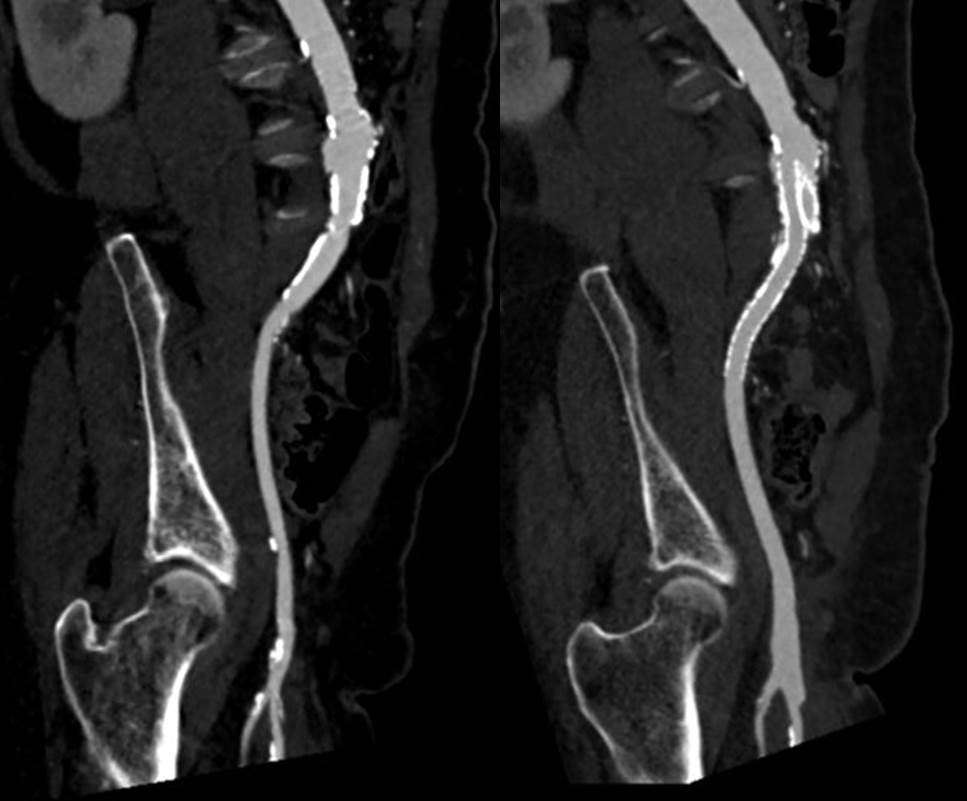
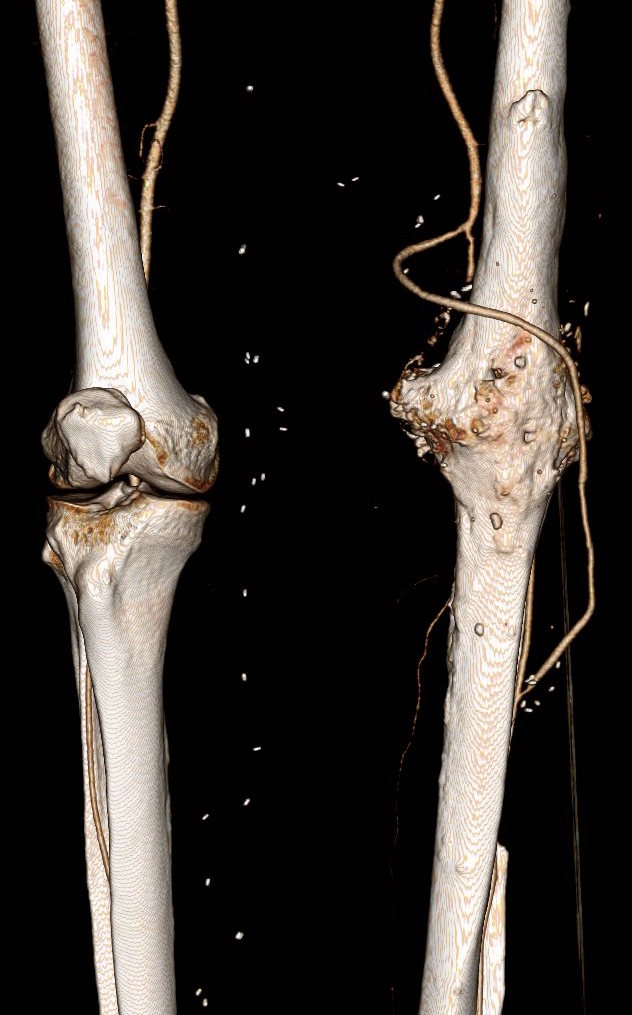
The other interesting finding was that he had an abundance of very good vein. Following surgical dictum, his original and subsequent surgeons had used his vein from his contralateral saphenous vein. His right leg, fused at the knee, lacked a good calf muscle pump action. While there were no varicose veins, the greater and lesser saphenous veins were large and generous conduits, at least by 3DVR imagery, confirmed on duplex (image below, white arrows).

The extant arteries were smooth and plaque-free. I decided to harvest his lesser saphenous vein and through the same incision expose his distal superficial femoral artery and tibioperoneal trunk. While I anticipated some scarring, I was confident that the sections of artery I wanted to expose were easy to access because of some distance from the fused knee.
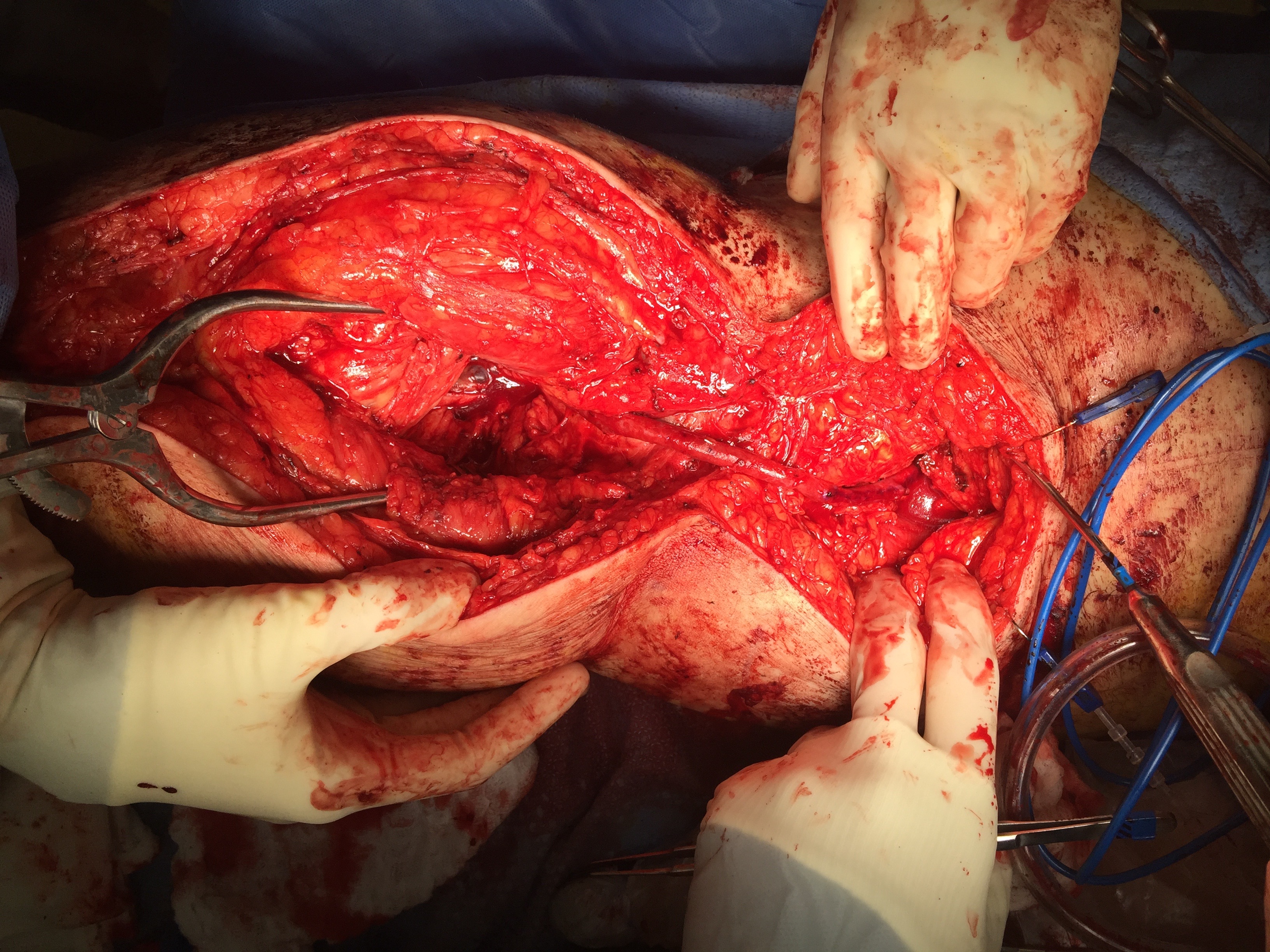
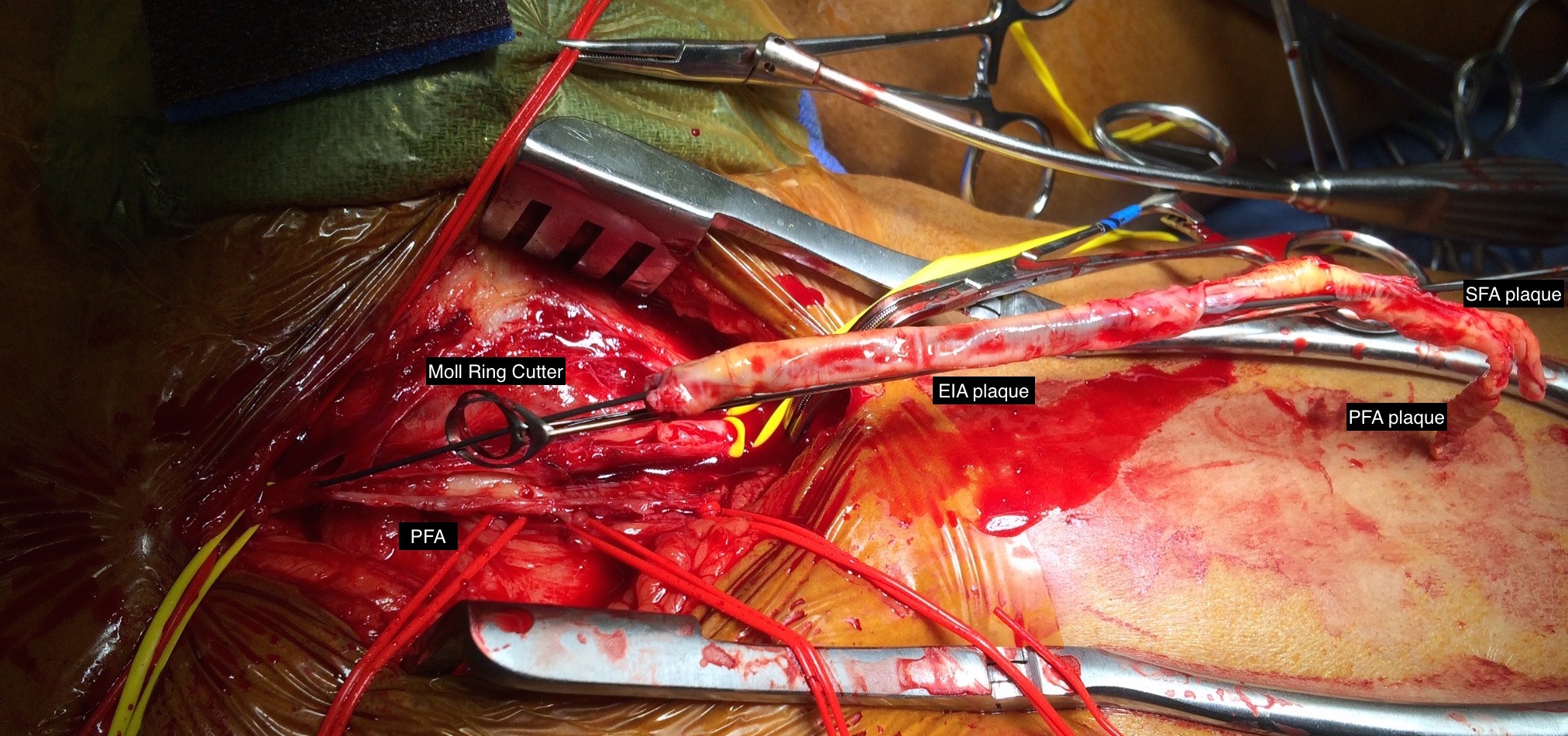
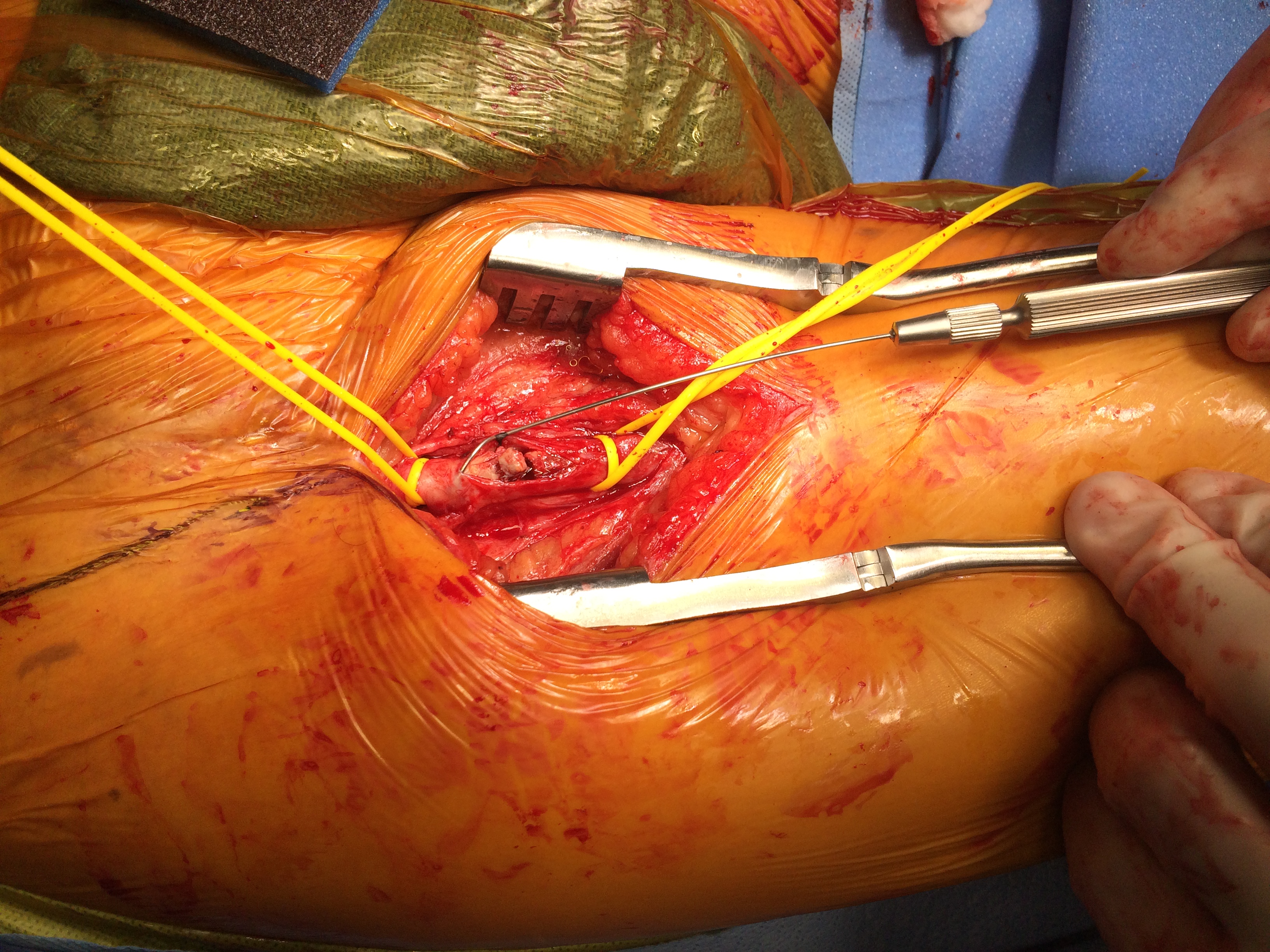
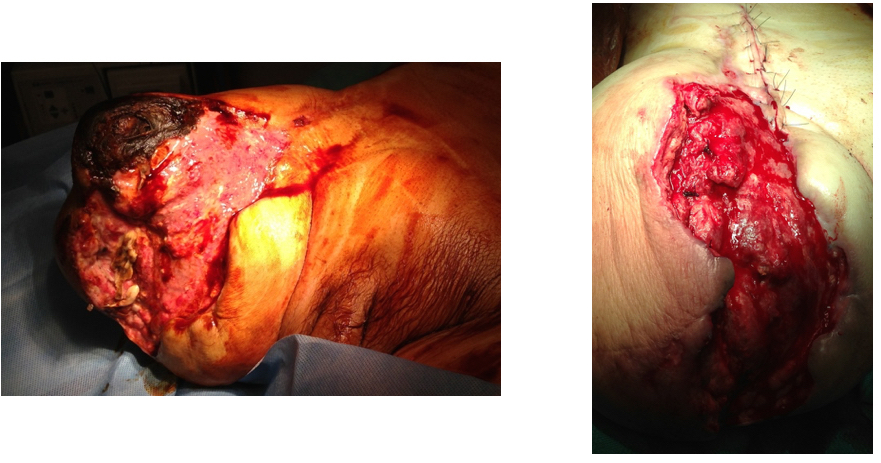
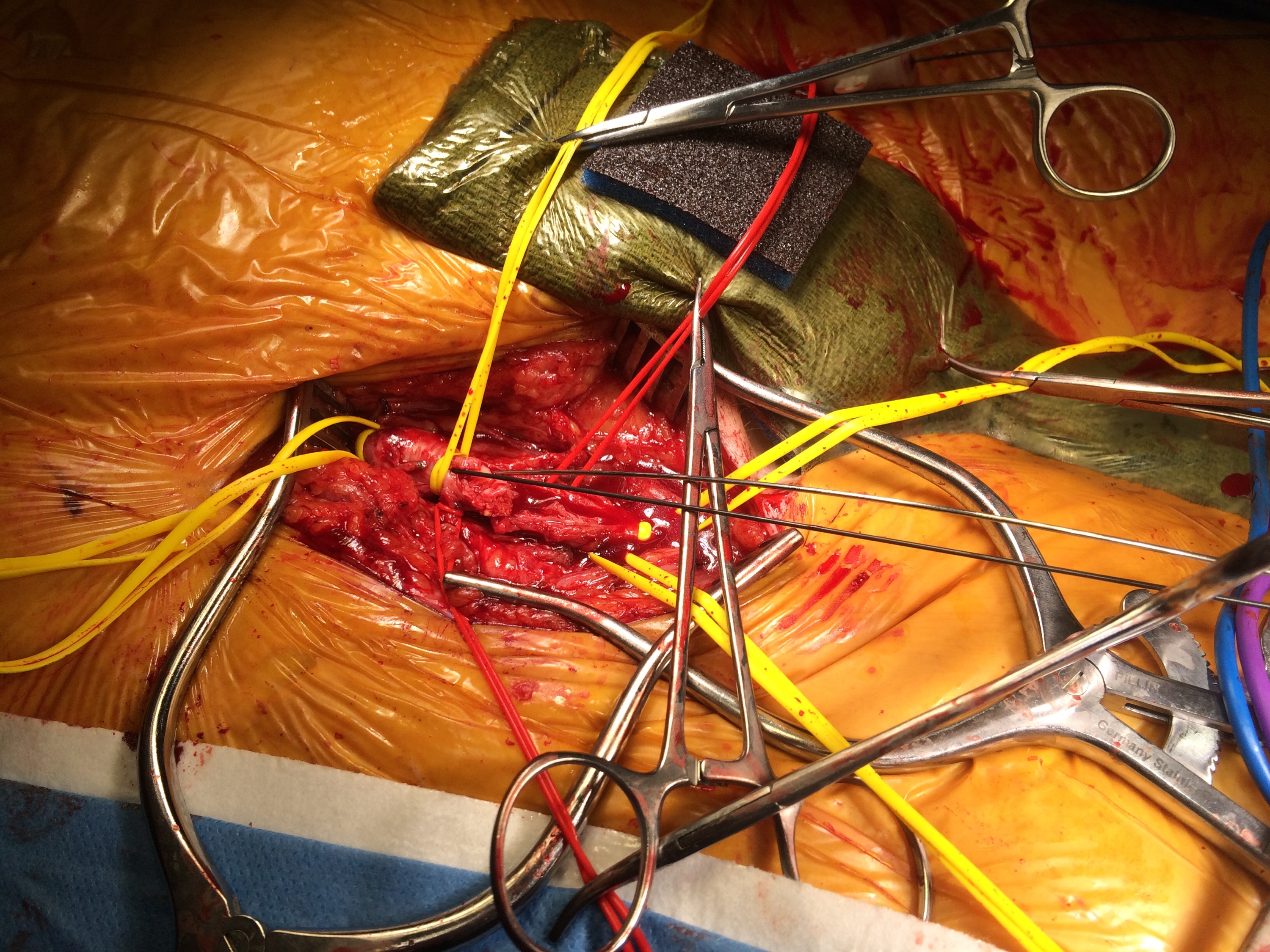
The picture shows the exposure and reversed vein graft in-situ, using the segment of lesser saphenous vein. As in prior experience in redo surgery, you can never know if a dissection will be easy or hard simply based on fear or concern for breaking something. It’s not until you start bushwacking –carving through scar and dealing with extraneous bleeding will you learn whether it was easy or hard. You can only be certain it was necessary. The only hitch was the femoral artery while well exposed, was buried in scar, and I chose not to get circumferential control as I was fairly deep, and had avid backbleeding from a posteriorly oriented collateral that required a mass clamp of the deep tissues.
Will this work better? Don’t know but it has a good chance, and I think a better chance. It is a large vein oriented in a straight path over a short distance going from good artery to good artery. This is better theoretically than a long meandering bypass with smaller vein.