My list of favorite things this year is simpler than in the past, in respect for the difficulties of the past year. Everything is under $300, and I use these every day. Treat your surgeon well and she will give you a nice scar.
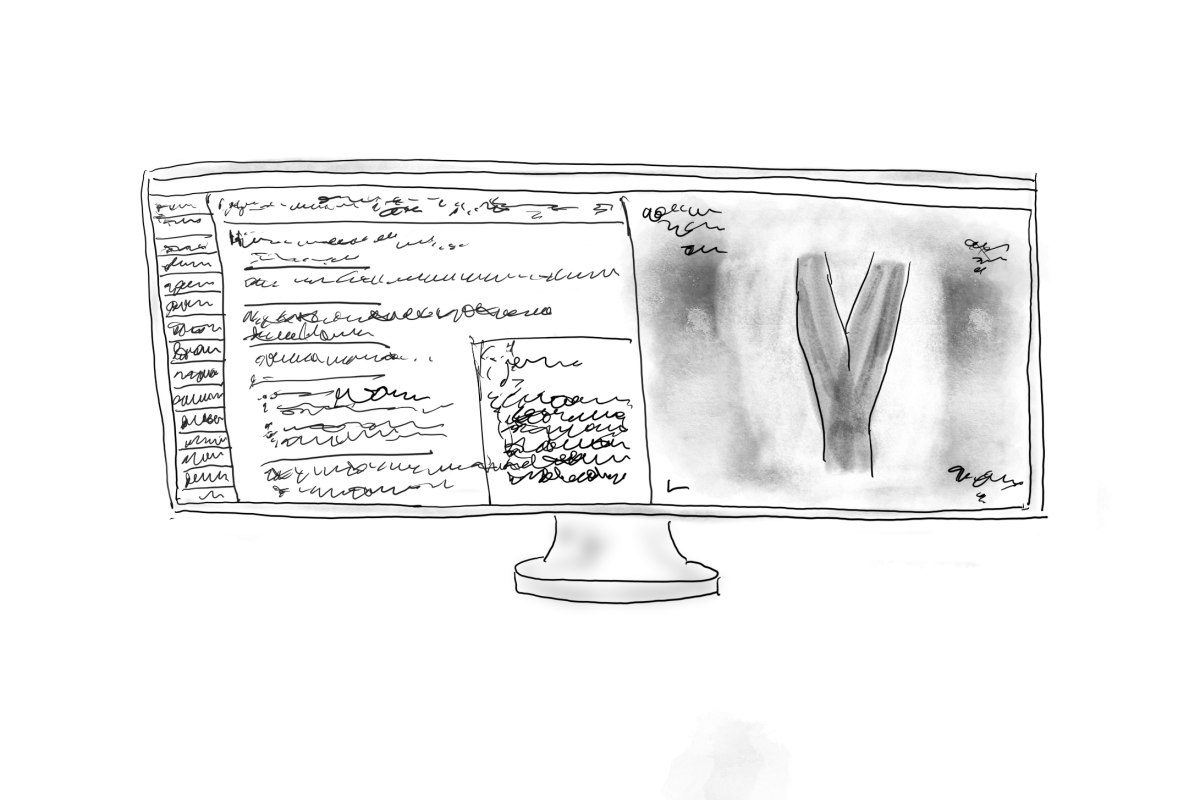
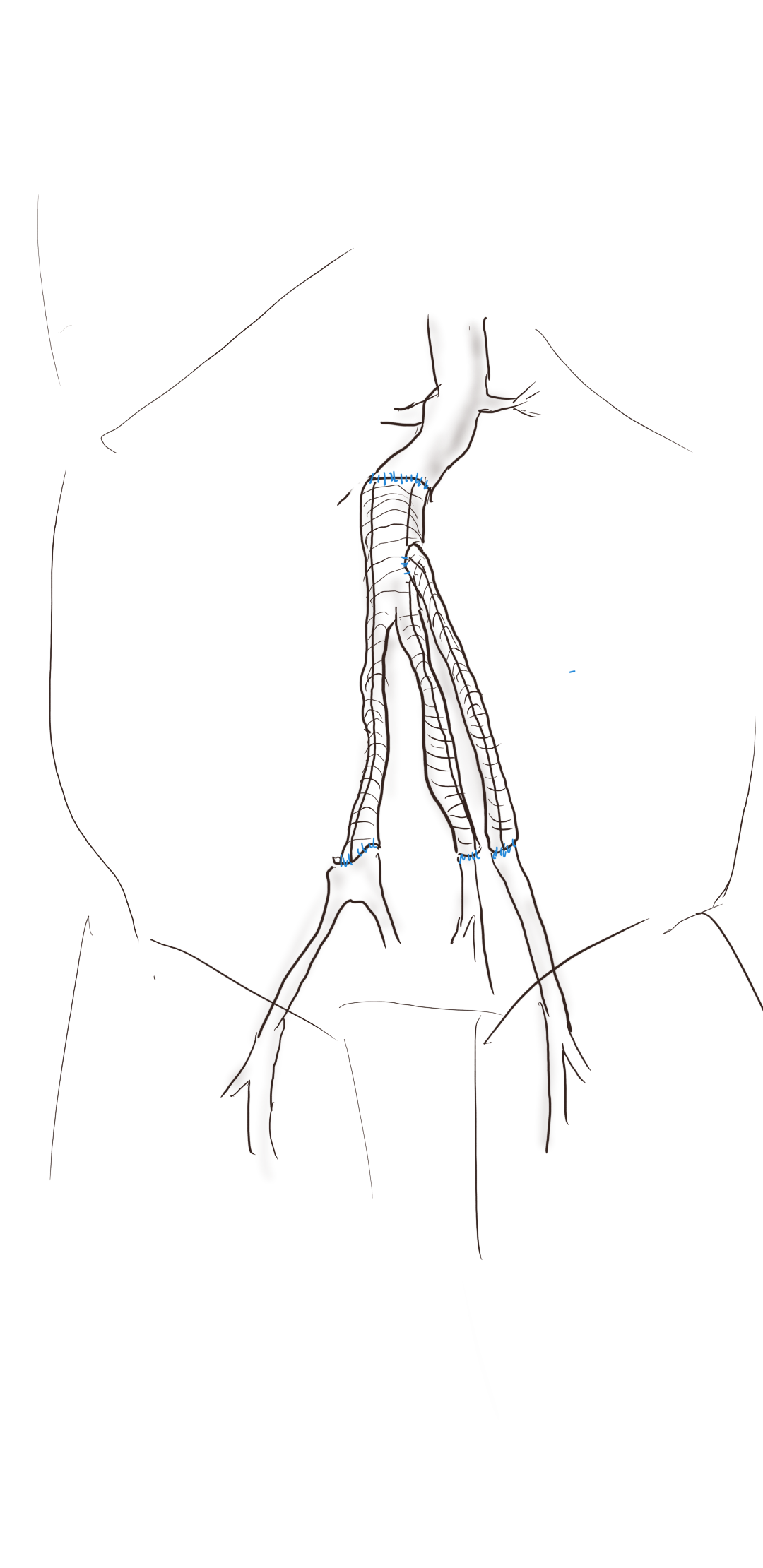
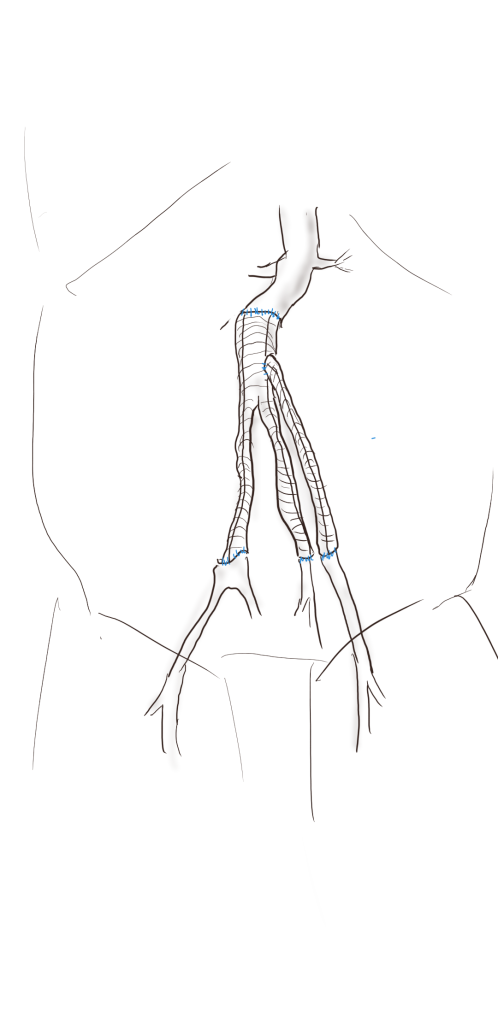
1. Lenovo Ideapad Duet. Cloud computing has diminished the need to carry processing power unless you are editing Pixar films or playing super high resolution video games. For composing words on the go, and sketching diagrams for patients, and putting together powerpoints, this Chromebook hits the sweetspot of price, battery life, and quality. It comes with easel stand and attached keyboard with trackpad. An Apple Magic Keyboard for the iPad costs more than the Duet! Battery life is easily all day, and in tablet mode, streaming movies is great. It fits on the stunted traytables on airplanes well because of its petite size. I drew this sketch for planning an arch repair on it. Can’t beat the price at $249 and cheaper with discounts. I got mine as a open box at Best Buy for $200.
Sketch made on a Lenovo Duet
2. Theragun Mini. It is a stereotype that middle aged Asians buy giant massage chairs, which are AMAZING, but if you want something more manageable, the Theragun Mini is the ticket. It is a personal massager designed for deep tissue massage, with a lithium ion battery built in. After a long day of operating, all the aches are pulverized by this machine.
Theragun Mini
3. Masterclass Subscription -During pandemic, diversions like enrolling in an MBA program and Youtube yoga, are the hot ticket, but for someone with a short attention span in need of non-work diversion, these classes are great! Penn and Teller teach magic. Steve Martin teaches comedy. And FBI hostage negotiator Chris Voss teaches high stakes negotiation. All of these highly relevant to a vascular surgeon. Trust me.
4. Moleskine Backpack -I have struggled with overly heavy work bags, but need to carry my computer and some papers and maybe a water bottle, pens, a powerbank, some cables. I find black vinyl laptop bags generally horrible to look at, and too easy to overpack. Expensive leather designer bags carry a similar price as a handbag from Gucci or Louis Vuitton, and would not survive a day without getting scuffed. This backpack from Moleskine, yes the notebook company, is both beautiful to look at but practical as well. It is water resistant and holds everything I need for the day. Has a measured number of compartments and inner panels for pens, cables, and cards, and is well padded for carrying your electronics. Looks great, and would survive medical school.
Moleskine Backpack -not just for notebooks
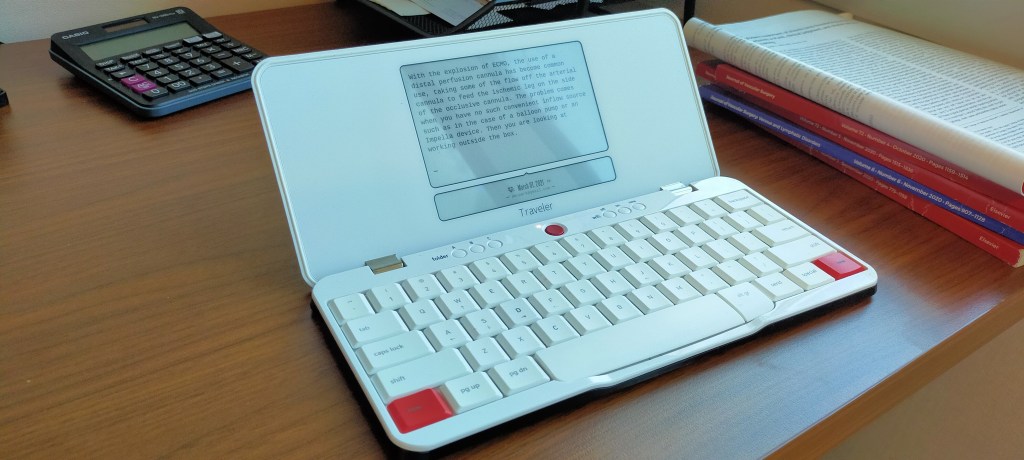
5. Freewrite Traveler -a writing appliance, a typewriter. The original Freewrite was designed to look like a typewriter, and the spirit of the machine is it takes away all the distractions of the internet for the focus of plain paper. The Traveler is the second machine by the Freewrite people, and offers the same focused writing in a portable package. Not for everyone, this one, but if you like writing, if you must write, this is amazing. It features a Kindle-like e-ink screen, and you type without the ability to edit. Everything you write goes to the cloud of your choice, including Dropbox and Drive, and so you won’t lose it. It has internal space for thousands of pages, and a 4 week battery life. If you hope to write the Great American Novel, this is the gadget for you.
Freewrite Traveler for the Hemigway in you
6. LED UV Blacklight -If you’re of a certain age, Spencer’s Gifts was one of the stops you made at the mall, and you always checked out the blacklight section, with its fluorescent posters and purple lamps that made your white shirt glow. As a surgeon, you want a Wood’s Lamp, but most hospitals do not have one, and most nursing staff have no idea what you are talking about. Good thing is that there are many cheap but powerful LED Blacklight options that emit UV light. This is great to have in the OR for a fluorescein test of gut perfusion (link). Take it camping in the deserts around here and you can see the scorpions at night! Or you can torture yourself by breaking it out at the next hotel you stay at and visualize all the glowing “protein stains.” Under $10, but slightly more for the higher power ones.
portable LED blacklight!
7. Old School iPod -This is as close as you can get to getting a Walkman without dealing with the inconvenience or poor sound quality of cassette tapes. In 2004, these were cutting edge, and Apple to its credit still supports file transfers of purchased (but not streaming) music files. The cool thing about these is that if you can do a carotid endarterectomy, replacing the battery and upgrading the memory are nothing, and there are many videos on line to show you how. These units are cheap to find on eBay, and there is nothing cooler than carrying around 10,000 songs in your pocket, without the need for a network, meaning uninterrupted music in the OR without relying on the network.
An iPod I purchased in 2006, upgraded to 32gB from original 8gB, just replaced battery for third time, still works.
8. Golf Ball Stamps -These stamps are meant to mark golf balls, but they are incredibly useful for graphically marking up a printed list. Each of these symbols represents a status or an action, which lets me look at a list at a glance and remember exactly what needs to happen. At pro shops everywhere.
Meant for golf, repurposed to act as semiotic markers on lists
9. Swiss Army Knife -the first one I got was as a graduation gift from my dad, thought technically not a gift as superstition dictated I purchase it from him for a dollar, it was the same as this one which is currently my fourth, bought at a Boy Scout camp for about $10. I keep one in my checked luggage for use at my destination for opening bottles, uncorking wine, cutting salume and cheeses, tightening screws, and when the occasion arises, performing an appendectomy (need a hotel sewing kit). This one also has tiny forceps and a toothpick.
With this, I can do several life saving operations.
10. Skirt steak -rarely seen any more shrink wrapped at chain groceries, you generally have to ask the fellow behind the counter or know a butcher. This diaphragmatic muscle used to be cheap. Considered offal in many places, this formerly cheap meat ended up being the go to meet for tacos and street cart barbecues in Asia, but don’t sniff at it. As it is not a structural muscle, it is not tough, has great flavor, and while leaner than traditional steak cuts, not devoid of fat like a filet (which is not my favorite) giving it enough buttery fat tones to remind you it is meat. Because it’s harder to find, that means the people who supply it know beef. Here in Abu Dhabi, I ordered this from the CarniStore in Dubai. Dinner is served.
The patient is a young woman who presented with classic symptoms and findings of median arcuate ligament syndrome (MALS). She avoided food because eating triggered severe pain in her upper abdomen. Over a year, this resulted in 15 pounds of weight loss. As a result, she no longer had the energy to work or exercise. She had an extensive gastrointestinal workup including blood work (LFT’s, amylase, cholesterol panel), abdominal CT scan, and upper endoscopy which were normal except for the finding of narrowing of the celiac axis due to compression by the median arcuate ligament. Examination was notable for upper abdominal pain exacerbated by pressure and seated, hunched-over posture. Unfortunately, due to her health insurance, surgery was not covered and she did not want any. So I recommended she try the following.
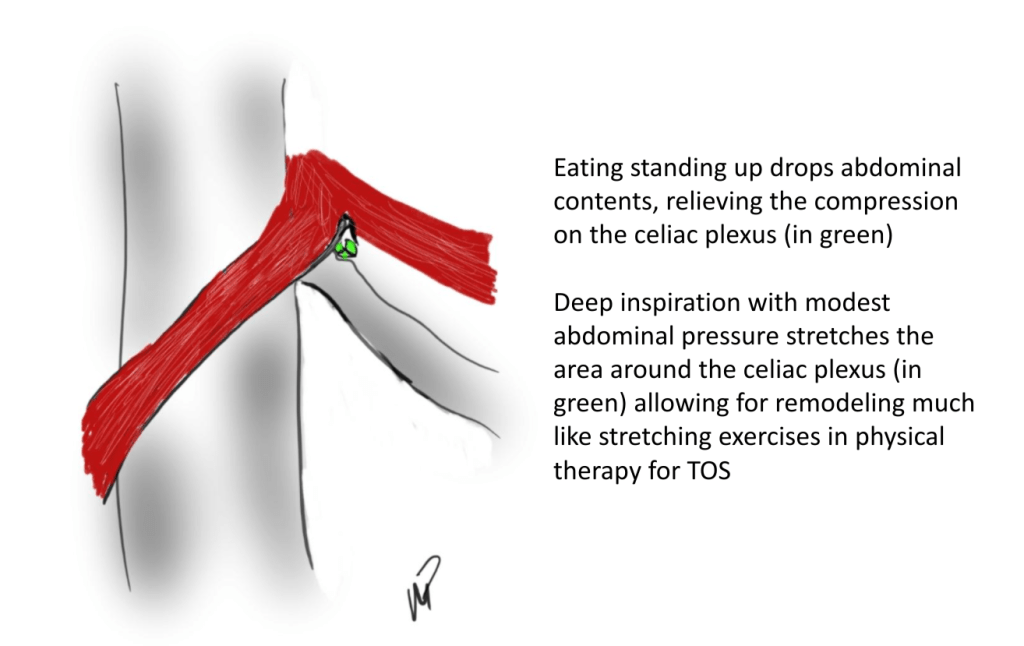
Eat standing up with good posture, shoulder back, back arched, taking deep breaths and holding once food passes
Practice upward facing dog yoga pose (figure) 5 reps daily with deep inhalation breath holds. If this is difficult, do this standing up.
Improve the posture during seated work, never hunch over and pressed forward with “shrimp back,” periodically take a deep breath and hold with excellent posture.
Upward facing dog yoga pose -shoulders square, outward collar bone tension, with deep inhalation breath holds
Over the past several years, I’ve noted that most patients respond to this, even in acute MALS pain situations (yes, there is acute MALS like slipped discs, for another post). That patient came back a few weeks later reporting that she was able to eat more food, more frequently. She also acknowledged compliance with the exercise and postural adjustments at work. A month later she reported regaining her lost weight and only mild pain with sitting in a car for a long time. She was still eating standing up, and she was grateful for having been treated without surgery.
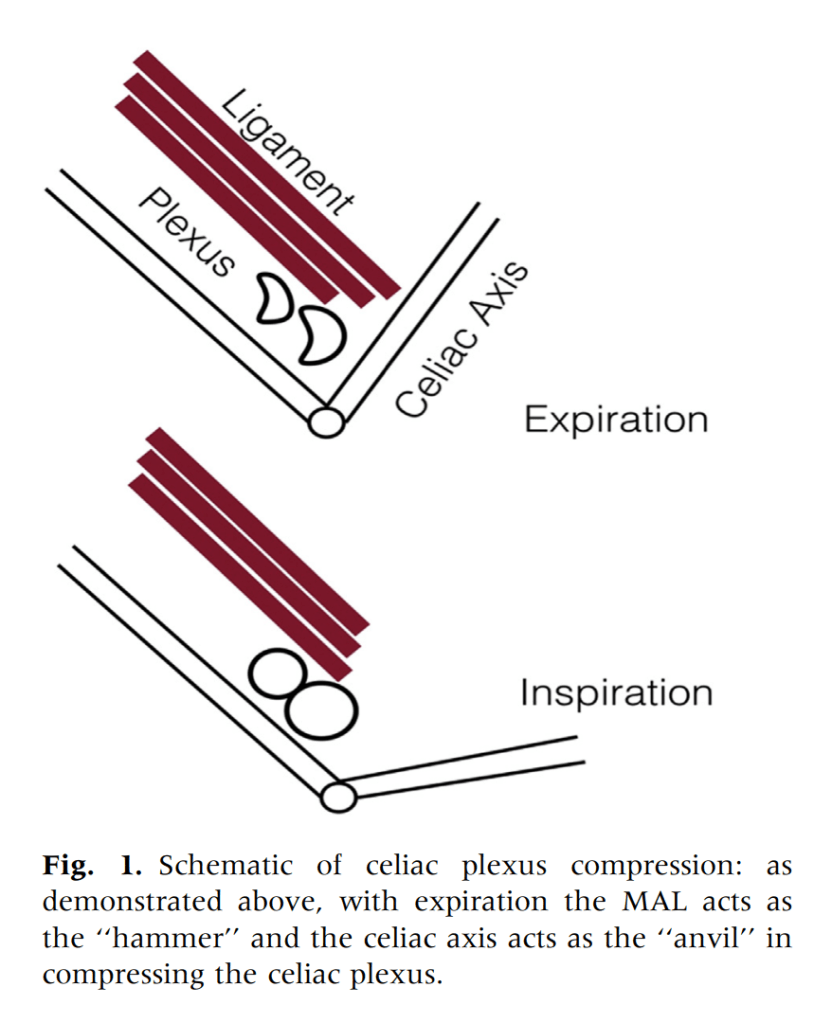
From reference below, a mechanism for celiac plexus compression, injury, fibrosis, and development of neuropathy
We have postulated that MALS is a nerve compression syndrome of the celiac plexus by the median arcuate ligament (reference). There are two consequences to MALS, neither of which is mesenteric ischemia. The first is this compression of the celiac plexus with injury resulting in inflammation and fibrosis, resulting in further compression and a neuropathy of the celiac plexus. This neuropathy triggers aberrant pain sensations in response to eating. The other consequence is remodeling and injury due to arterial compression. The celiac axis can develop post-stenotic dilatation, growing large enough to be considered aneurysmal. The compression can damage the intima resulting in dissection. The artery can be injured and a pseudoaneurysm can develop. Finally, the aneurysmal segments may develop thrombosis and be the source of thromboembolism, usually to the spleen. Even when the celiac axis clots off, unless there has been resectional surgery such as a Whipple or splenectomy, the stomach gets enough collateral flow that ischemia is rare when celiac axis occlusion occurs. So similarly to thoracic outlet syndrome (TOS), there is a neurogenic MALS and an arterial MALS.
The first line of therapy in neurogenic TOS is physical therapy. With symptomatic MALS, I wondered if there could be physical therapy as well. This young woman and others I have managed nonoperatively suggests good response in some, and partial response in most to exercises and maneuvers designed to address the compression.
Currently, in lieu of celiac plexus block, I have patients treat their MALS nonoperatively using the above protocol for 2-4 weeks, typically while they undergo further workup to rule out more common gastrointestinal etiologies of their abdominal pain, and many have been able to improve their circumstances with these measures alone. This patient chose not to have operation as she was able to live symptom free and regain lost weight with these recommendations alone.
Addendum
I received a comment from Ms. Suzanne Peek, president of the National MALS Foundation, who correctly pointed out not everyone presents in this way. I agree each patient undergoes a unique journey that is often marked by diagnostic delays because this is a rare condition. As I stated, not every patient responds to this regimen and after work up typically will undergo surgery to which in our published results 85% have a positive response to when diagnosed with MALS. Is certainly an area of further study to see if more people can respond to this non-operative approach. Our previous protocol which we instituted after the publication of our report was to use celiac plexus blockade as a diagnostic study and occasionally permanent blockade as therapy for those with prohibitive operative risk. A positive response to this regimen may signal a positive response to surgical celiac plexus ablation.
Reference
Weber JM, Boules M, Fong K, Abraham B, Bena J, El-Hayek K, Kroh M, Park WM. Median Arcuate Ligament Syndrome Is Not a Vascular Disease. Ann Vasc Surg. 2016 Jan;30:22-7. doi: 10.1016/j.avsg.2015.07.013. Epub 2015 Sep 10. PMID: 26365109.
Every once in a while, I will make an exception to the SVS guidelines on AAA repair with regard to size at time of repair (link). I have a bunch of excuses. When I trained in 2000-2002 with several giants of vascular surgery, there was some controversy when the first guidelines came out in 2003 (link). The board answer became 5.5cm that year, but where I trained, it was a minority opinion held by Dr. Jeb Hallett. The majority was in the belief that as long as operative mortality was low, even high risk AAA repair could be undertaken (link). The published risk for Mayo was low, and that came from both technical excellence and high volume (more on that later). The criteria during my fellowship was 4.5cm in good risk patients for open repair based on data generated in the 1980’s and 90’s during Dr. Hollier’s tenure.
Then as now, the debate centered around the balance of risk. At specialty centers that achieved less than 1% mortality rate for elective open AAA repair, 4.5cm in good risk patients would seem perfectly reasonable. But given the 5-10% mortality seen in the Medicare database at that time for community practice, the 5.5 cm criteria was not only good science, it was prudent. The first set of guidelines held off the contentious volume recommendations that was the nidus of conflict within other surgical societies.
The advent of endovascular was a game changer -the mortality rate in the Medicare databases was 1-2% for EVAR in the community setting, meaning more surgeons in most hospitals could achieve tertiary center levels of mortality with this new technology. The issue was never really settled in my mind through the 2000’s, even with the PIVOTAL Study. I enrolled patients into the PIVOTAL Study (link) at that 4.5cm threshold during my time in Iowa. Eventually I lost equipoise and I stopped enrolling after a handful of patients. It had to do with graft durability.
Around that time, I took two patients in a row to the operating room for sac expansion without identifiable endoleak. They were Dacron and stent-based endografts placed about 5-7 years before by another surgeon and aortography failed to show type I or III endoleak. Sac growth was over a centimeter in 6 months and the aneurysm size was over 6cm in both. I chose to marsupialize the sac and oversew any leaks, with the plan to replace the graft if there was a significant leak. On opening the sac, no significant lumbar or IMA leaks were encountered but in these patients a stream of blood could be seen coming from the sutures securing the stents. It was the same graft that was in the trial, the AneuRx, and that was when I realized that these grafts have the potential to fail in the same way that patio umbrellas leak after years of use -cloth sewn to rigid metal with movement wears open the cloth wherever there is stitching. This did not happen with open repair. I lost enthusiasm for the trial as I lost faith in this graft which was retired from the market. I placed pledgetted sutures to close the leaks on both patients, and closed the aneurysm sac tightly around the graft in one patient who was higher risk, and replaced the stent graft in the other.
There are some exceptions to justify repair of 4.5-5.5cm AAA. During my time in practice, there were patients who lived far away from major medical centers who would not survive a ruptured AAA even if the rupture rate was low and who confessed they only came into town every five years or so. There were patients who suffered from clinical anxiety whose AAA was documented by a psychiatrist to amplify their anxiety. There were patients with vague abdominal pain for whom thorough workup have ruled out gastrointestinal causes and every visit to the ER triggered a CT scan to rule out AAA rupture. And there seemed to be some patients who seemed to have such perfect anatomy for EVAR, whose risks were low, and whose growth rates were so consistent that their repairs could be timed on the calendar. Some combination of these factors and lobbying on the part of the patient got them their repair in the 5cm range. And they still do.
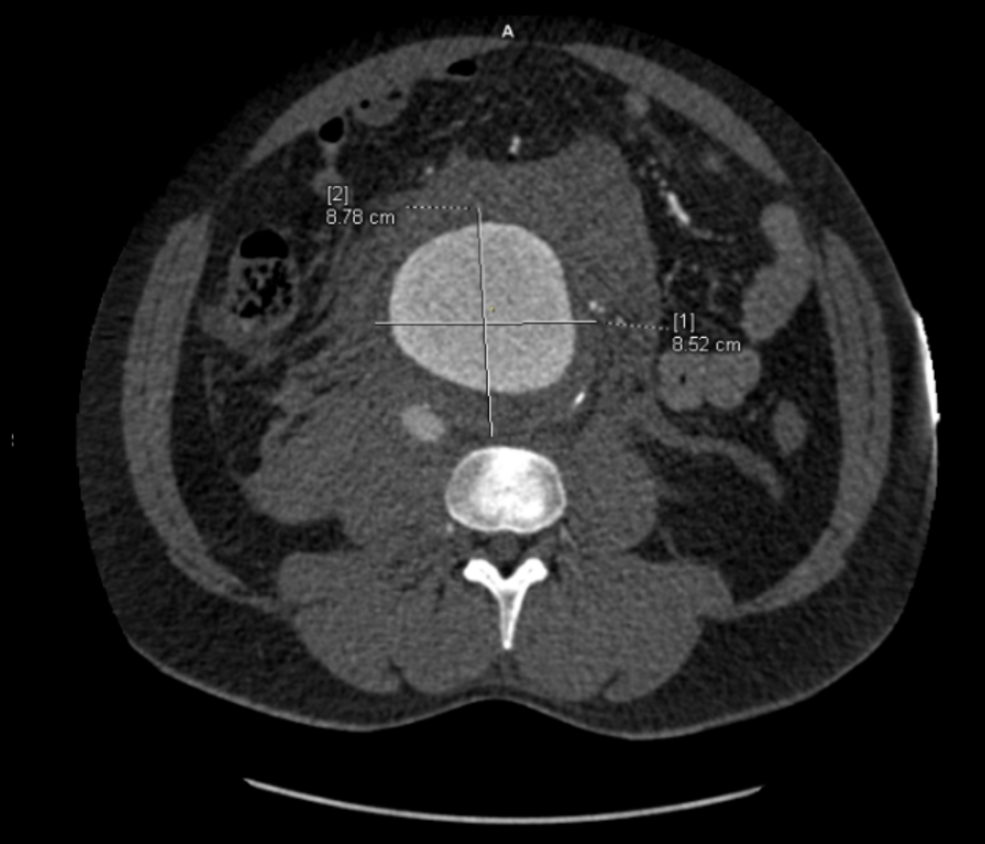
The patient is a man in his sixties with hypertension who presented with a 4.7cm AAA which in various reports he came with described 5.2×4.7cm. After review of his images, it was clear it was 4.7cm. If measured on a typical axial cut CT scan or a horizontally oriented ultrasound probe, a cylindrical aortic aneurysm will be seen as an ellipse in cross section. A radiology report will typically report an aneurysms length and the anteroposterior and lateral dimensions. If you cut a sausage at an angle, the ovals you cut can be quite wide but the smaller length of the oval reflects the diameter of the sausage.
Looking back at his records, for three years he had multiple CT scans for abdominal pain showing the AAA and a well documented record of growth of about 2-3mm annually -the normal growth rate. He asked me to prognosticate and so I relayed that 4.7cm in 2017 with a 3mm growth rate, we would be operating in 2020. The anatomy was favorable with a long infrarenal neck and good iliac arteries for distal seal and access. He was quite anxious as whenever he had abdominal pain, his local doctors would discuss the AAA and its risks or order a CT. After a long discussion and considerable lobbying by the patient and family, I agreed to repair his 4.7cm AAA.
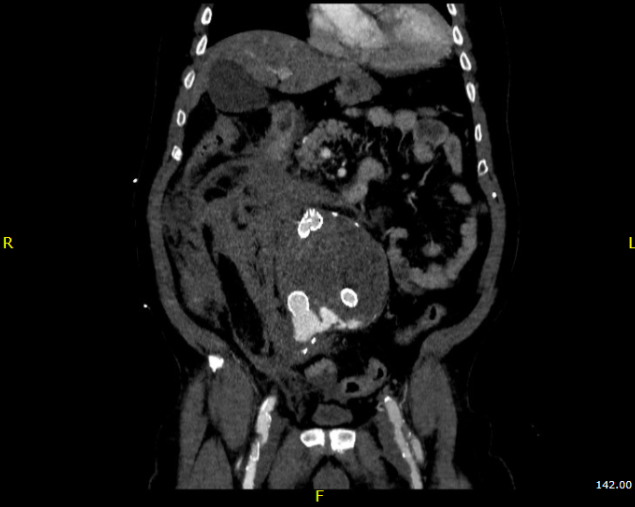
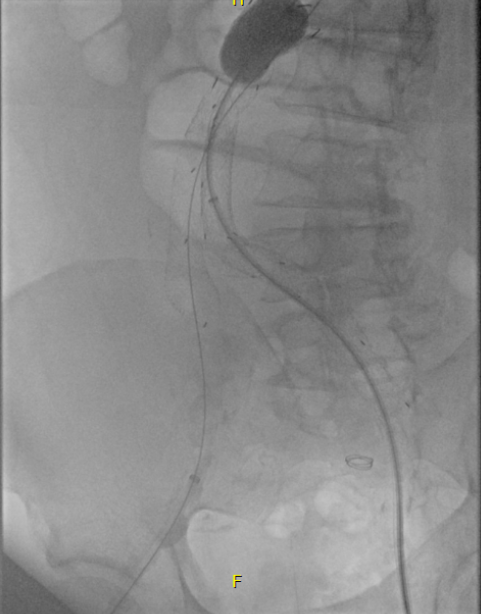
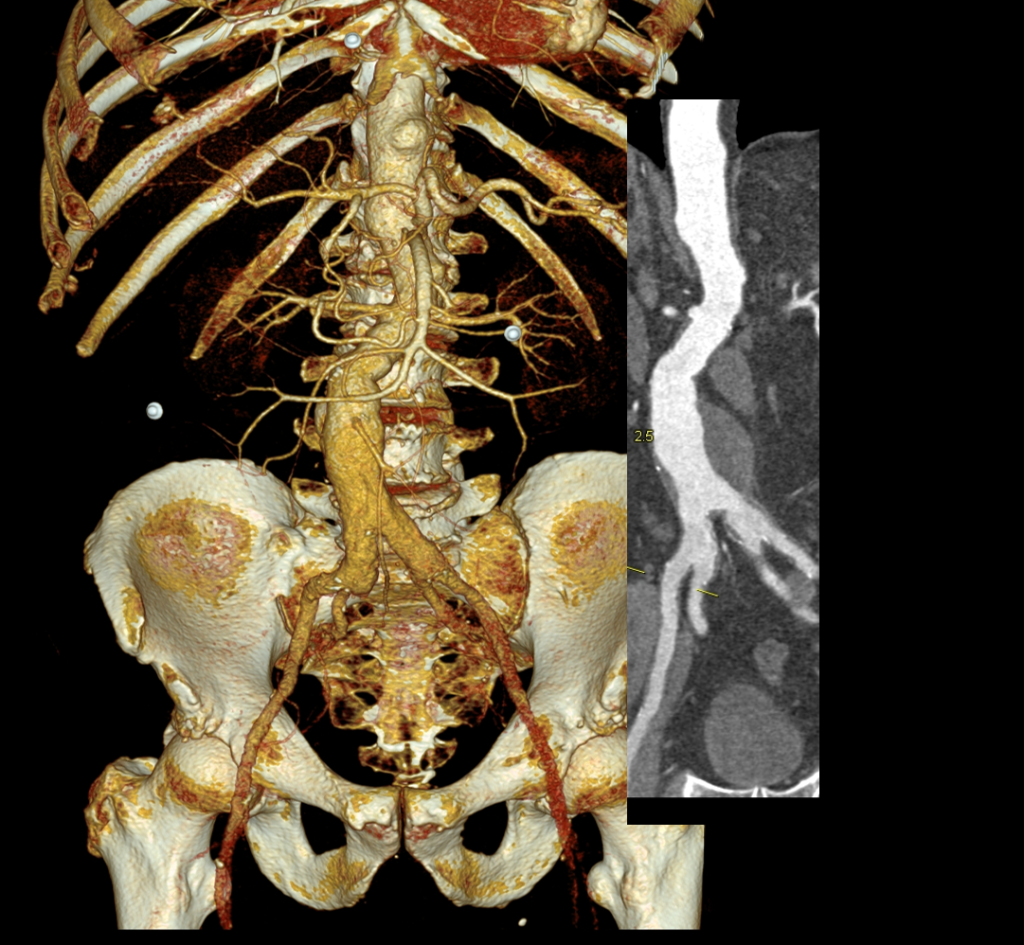
The EVAR was performed percutaneously. No endoleak was detected by completion arteriography (figure). He was soon discharged and was grateful. In followup, CT scan showed excellent coverage of the proximal and distal zones and absence of type III endoleaks. There was increased density to suggest a type II leak, but his inferior mesenteric artery was not the source of it. over a three year period, his aneurysm sac continued its 2-3mm of annual growth despite the presence of the the stent graft.
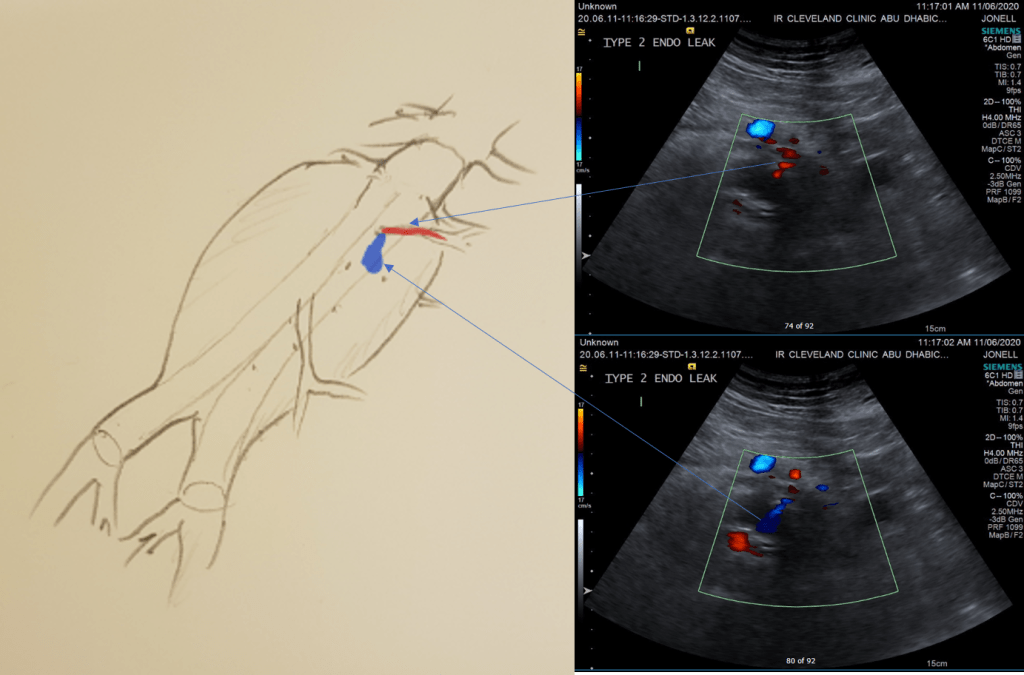
While CT failed to locate this endoleak, abdominal duplex ultrasound did showing flow from a small surface vessel (duplex below, figure at beginning of post). It was not the inferior mesenteric artery which can be treated endovascularly (link) or laparoscopically (link). CT scan suggested that it was one of those anterior branch vessels that one would encounter in exposing the aorta. Usually these were higher up as accessory phrenic arteries, but these fragile vessels, larger than vasovasorum, but smaller than named aortic branches, are seen feeding the tissues of the retroperitoneum.
Ultrasound revealed the type II endoleak from an anterior retroperitoneal branch artery.
Type II endoleaks are not benign. The flow of blood into the aneurysm sac after stent graft repair is almost never benign. It is a contained hemorrhage. There are three components to the pressure signal seen by the aortic aneurysmal wall that could trigger breakdown, remodeling, and aneurysm growth. They include pressure, heart rate, and the rate of change of pressure. The presence of fresh thrombus may play an inflammatory role. Some endoleaks clearly have a circuit and others are sacs at the terminus of their feeding vessels, never shutting down because the AAA sac can both accept and eject the blood flow. Changes in AAA sac morphology due to sac growth can cause problems with marginal seals, component separation, and component wear. Sac growth can cause pain. Ruptures, while rare, can cause death. Mostly, type II endoleaks generate more procedures because it is hard to ignore continued growth.
Review of aortogram from device implantation showed a small anterior artery arising from the proximal aortic sac (arrow)
Three years of followup showed growth of the AAA sac to 5.5cm, which ironically threshold for repair. Again, no type I or III endoleak could be seen. He reached his calculated repair date, and I discussed our options in detail.
1. Do nothing, keep following
2. Endovascular attempt
3. Open surgery, marsupialization
4. Laparoscopic ligation of target vessel
Doing nothing hasn’t worked for 3 years. What would more time buy? Endovascular -to where. The IMA is the usual target for an endovascular attempt, although iliolumbar access is possible (link), we really needed to fix this with one attempt. Open surgery is a great option -a short supraumbilical incision is all that would be needed to open the AAA sac and oversew the collaterals. The patient did not want a laparotomy. There are reports of laparoscopic guided endovascular access with endovascular coiling of the remnant sac with fluoroscopy. This adheres to the letter of the claim of minimal access, but really?
I compromised with the patient and offered laparoscopy. I have ligated the IMA a handful of times laparoscopically -these are relatively fast and straightforward cases. As I had the location of the endoleak, I felt it should be straighforward to dissect out the anterior sac much as in open repair and clip this vessel.
Use of ultrasound allowed localization of the leak and identification of the artery for clipping.
Of course, what should have been a 30 minute procedure through a minilaparotomy became a two hour enterprise getting through scar tissue (not the first time encountering this after EVAR) while pushing away retroperitoneum. I recruited the help of general surgery to get extra hands, but the patient was well aware that there was a good chance of conversion. Patience won out as the artery was ultimately clipped and endoleak no longer seen on ultrasound.
I waited a year before putting this together as I wanted CT followup. The sac stopped growing and has shrunk a bit back to 5cm or so. There will be those who argue that nothing needed to have been done about this leak as it would have stopped growing eventually, but I would counter that an aneurysm sac that kept growing like the stent graft never went in is one demanding attention. The key role of duplex ultrasound cannot be minimized. We have an excellent team of vascular scientists (their title in Europe), and postop duplex confirmed closure of the leak.
Not seeing the leak anymore is a positive, but the stent graft remains.
The patient is quite satisfied having avoided laparotomy. His hospital stay was but a few days. During my conversations with our general surgeons who are amazing laparoscopists, that this would have been a nice case with the robot. That’s a post for another day.
The definition of success in this case and many EVAR’s plagued by type II leaks leaves me wondering. Excellent marketing of the word “minimally invasive” has subtly defined laparotomy as failure, and not just in vascular surgery. When costs and efficacy are reviewed as we come out of this pandemic, I suspect that open surgery will selectively have its day in the sun. A ten blade, a retractor, a 3-0 silk is so much more cost effective than five ports and disposable instruments. And a stent graft system?
The Long of It and the Short, or What You Are Trying to Do With That Level 82 Note on Your EMR?
I struggle to keep my sanity reading through electronic medical records. Medical billing pays by the amount of note written. Back in the 90’s, the insurance companies demanded that paper records be sent by mail or fax to confirm billing. Clerks in medical records departments would spend the whole day copying and faxing stacks of charts to payers and billers. EMRs were suppose to solve this, but the paradigm of the paper record lives on. Each note in the EMR is printable as a paper record for billing. It is a static text document. And like in the 90’s, billing is based on the amount of note written into the EMR. The simplest way to achieve this is to copy and paste what already exists elsewhere in the EMR -a past note, a systems review, a medical history, a spreadsheet of lab results, imaging reports. This gets you more note, more billing. The electronic medical record succeeds in its primary function as a cardboard box of copied records and as a cash register, but fails miserably in being an active part of patient care.
Any sane system would allow you to pick links to prior notes or tests -a referencing system to include even published articles, to show your logic and data, while allowing you to focus on the information that is important at the moment. The modern note needs to be turned into a searchable, linkable, living element in a dynamic database reflecting the patient’s status, a powerful tool in the patient’s care. There needs to be an App Store where third party vendors can craft solutions not imagined by the EMR. There needs to be a common file format to allow for interoperability and easy transfer of records between institutions -like JPGs and MPGs. There needs to be a complete re-engineering of the user interface. The various caregivers interacting with the EMR need to be allowed to input data in non-linear ways using mobile devices. The EMR needs to evolve to being a platform.
The Blue Ink
When I was a fellow in 2000, one of my staff, Ken Cherry, had this distinct light blue ink in his fountain pen that he wrote notes with in pithy, grammatically correct sentences conveying the diagnosis and plan. It was up to me, his fellow, to write the more detailed note, but there at the bottom, in a sky blue cursive fit for the Declaration of Independence, was the word. You just had to look for that ink in the chart to understand where the patient was and where he was going. He’d write something like, “This patient, who was seen in clinic with classic Leriche Syndrome, is now admitted with rest pain in his right foot. I intend to revascularize him after appropriate workup. My fellow will make these arrangements.” Stylistically, it was wonderful, but assumed a lot of contextual knowledge about Leriche Syndrome, and if you didn’t know, you could read Park’s two page note. He’s making the arrangements.
Compare that to an imaginary level 19 note (won’t burden you with it), rotten with copy pasted operative note and prior discharge summary, spreadsheet of laboratory values, and 12 system review of systems, 12 organ system examination, and multiparty listing of every organ in impression, bullet pointed plan, never mind that many of these have no relationship to the problem at hand. The first note is a financial disaster as it cannot be maximally billed, but it is full of meaning and action. The second note is unreadable and therefore likely unread. Like those strange tropical fruits that take power tools to get to a small bit of sweet at the center, the level 23 notes littering electronic medical records take time to pore over the chaff to get to the point which is often hidden -day to day only a few things may actually change on a note. There is just too much husk. Most of the action, the orders, have to be typed back into the note rather than automatically populating it. Supposedly, that function exists but the software has been written with the user interface of Windows from the early 1990’s and the functions are buried, only to be fished out by superusers and support staff that take time away from clinical duties to read about and learn.
Context Implied and Explicit
The fashioning of a good note recognizes that too much implied context results in confusion. Rather than say, “Leriche Syndrome,” one should say, “aortoiliac occlusive disease from advanced atherosclerosis resulting in a symptom complex of severe claudication known by the moniker, Leriche Syndrome.” The note needs to educate as much as it does document. The exposition of expertise needs to be explicit for the note to show value. Value and bill-ability do not live on the same axis. The reader should come away from the note with maximal meaning in the shortest amount of time. That means most consult notes and H&P’s need to be ideally case studies and earn their length and perform a teaching function.
Copy/Paste -Note as EMR Fractal
The position of the average physician is a poor one. The need to bill means writing long notes, but physically typing and formatting long notes is a drudgery that occupies a significant time away from seeing patients, performing procedures on patients, and thinking. The easy solution to this dilemma, the lack of time, is the Copy/Paste. There are notes where the entirety of past notes is copy pasted, creating a self-repeating element like a fractal where the entire EMR is reflected in the note. Like error mutations of the genes that persist and damage organisms, copying and pasting of documentation errors perpetuates itself and can cause disease. I remember years ago as a young staff being stuck by a needle during a procedure and dying a little inside when I checked the chart and found the patient was HIV positive. When I talked to the patient, I found out that was a persistent error, manually copied and pasted by residents and consultants, billed as a diagnosis, resulting in years of problems for the patient who had to threaten lawsuits to expunge that HIV status. Each note should be unique and uniquely authored by the caregiver, and if there is not much to report, necessarily brief. A daily summary should be generatable like those news apps that can scrape headlines and context out of the day’s production from the internet and present it to you in a easy to consume quadrilateral of data.
The Shield -Speaking to the Jury
A proper note will protect you. It is the only shield that protects you along with your education and reputation. Civil proceedings involve going over these notes in great detail and the notes should be either unimpeachably explicit or vague like a fortune cookie. Even the limited tech of current EMRs allows you to achieve granular levels of detail. I recommend referencing (but not copy/pasting) important societal guidelines and journal articles that reflect your thinking, but it the EMR does not make this easy. The hack is keeping these references as a macro to spew out relevant text. For example, if you chose not to operate on a 5.4cm AAA, after referencing the CT scan report, an image showing your measuring line, and the growth velocity from prior scans if available, a line reference to the SVS guidelines spat out by a macro gives you some shielding. But more important, in the ideal EMR, that reference would be that characteristic blue color of a hypertext link to the pubmed reference or PDF download. Hyperlinks within EMRs should be a thing. Your EMR note should be a hypertext document, not a text document, and allow referencing other notes and reports without copy/pasting them. Images, audio, and video should live within your EMR note as naturally as they do in every other document you create in 2020 that does not have to be excreted through a printer. The fact that these functions are extraneous to the primary function of the EMR -to be cheap to produce and maintain, and good for billing, means no innovation will occur for EMRs.
The Platform
EMRs vendors cling to their market share by making sharing of data impossible through proprietary data formats and security regimes. Health care systems have no incentive to make their patient information transferable beyond a minimum of paper or their PDF equivalent. Patient safety and information security is invoked for preventing needed innovation. For the patient, this can be a life or death issue -the ability to transfer health care data. Imagine if you are the patient with a ruptured aortic aneurysm who is transferred without the CT scan burned to a CD. In 2020, NO.ONE.USES.CD’s. I can download a 4K file of the last Avenger’s movie in 30 seconds on the right network, but a lifesaving CT scan -NO WAY!
A more everyday example is a patient seeking a second opinion or moving cities to a different health care system. The only way to move the data is an expensive printout of the chart. How can we keep this important information linked with the patient? Social media has cracked this. Your Facebook is a good model of what a potential EMR 2.0 could be. A patient-centric EMR would be controlled by the patient in terms of access control. Federal laws would prevent misbehavior by the EMR vendor. The patient’s data generated by practices or hospitals would be owned by these practices or hospitals but posted on the patient’s EMR, in specific specialty adapted formats. Temporal ordering would be natural, not based on shuffling reams of paper or virtually with PDFs with overlapping timelines. More importantly, imaging data and lab results would be immediately available to all healthcare providers through access to the patient’s EMR. Practices and hospitals would pay a nominal fee to the EMR provider much as advertisers are on Facebook. Patients would be in control of who gets access to the data, and importantly if they want to participate in research. App developers would proliferate and innovate in the space, providing functionality via apps in a marketplace, allowing different specialists look at the data in their own particular way, and patients to understand their data on their own terms. Gaming companies, for example, could take the virtual coordinates of a CT scan and match it up with ultrasound and MRI to do a lot of cool stuff. EMR 2.0 is not more ways to personalize your window with colorful graphics. EMR 2.0 is a complete upending of the way patient data is stored and moved, and it will take an act of Congress to make this happen. EMR 2.0 recognizes that it needs to become a platform and it needs to be a part of a collective national effort. EMR 2.0 needs to be a platform, not an app.
A Multimedia EMR
The EMR needs to incorporate multimedia. Current EMRs live in the tech levels of the early 1990’s. Imaging studies must live as actual windows in chart notes. Video or voice comments must be documentable in the chart. Hypertext to the resources of the internet must live in the chart. Data must flow just like blood.
This should suffice as an op note
Shape of the Future
As a vascular surgeon, the most important function is to provide an accurate documentation of the condition of the blood vessels to date, the current condition of the blood vessels, and the future fate of the blood vessels and the patient. Technology needs to help the vascular surgeon in this role, and most importantly, the patient. Tech is not a third party vendor in this battle space. Tech is a caregiver, and must be held to the same standards placed on physicians, nurses, and technicians. Until that day comes, we as vascular surgeons must write amazing, publishable case reports for the consult notes, and short pithy updates for the subsequent notes.
Narrow shoulders means the arm hangs off the first rib tethered by the brachial plexus
When Australopithecus began to walk upright, there were many consequences. It freed the hands from weight bearing, but it also burdened the shoulder girdle with the weight of the extremity. Boticelli’s Venus shows the Renaissance ideal of the narrow shouldered maiden, but that bulk of shoulder and arm meat and bone, roughly equal to the weight of a jamón ibérico (vacation pic below), hangs off the neck with pathologic consequences. Also, the australopithecine usually died by disease or trauma by the second decade if chimpanzees are to be believed, but we live for nearly a century wearing down tissues designed for 10-20 years.
jamón ibérico
Mechanically speaking, there is a weight and a rope. The brachial plexus is the rope and it is draped over the first rib. The muscles of the shoulder girdle should support the weight of the arm but with bad posture, another consequence of bipedalism, the muscles may not be up to the task.
When there is a cervical rib, the situation is worse. The thoracic outlet is narrowed, and the weight of the arm, the jamón, is borne on the cervical rib. The brachial plexus becomes stretched over this anomalous bone and the trauma results in symptoms of pain, weakness, and strange sensations. I am of the opinion that cervical ribs in general should just go when found as nerve (and arterial) injury when found late may be irreversible.
CASE
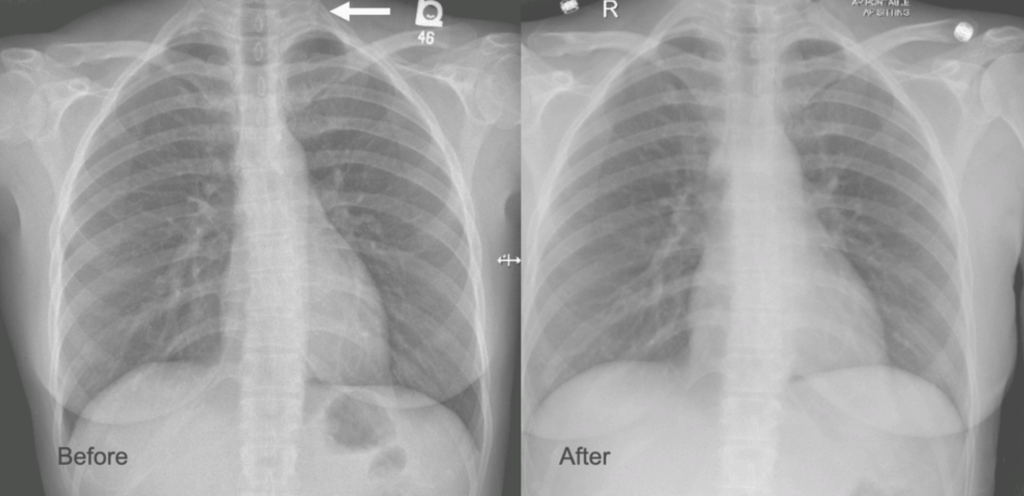
The patient is a younger woman who was referred from cardiology after workup of chest pain and left arm pain was negative for cardiac disease. She also had occasional right arm pain. The only finding of note during an extensive cardiac workup were cervical ribs found bilaterally on chest x-ray (below).
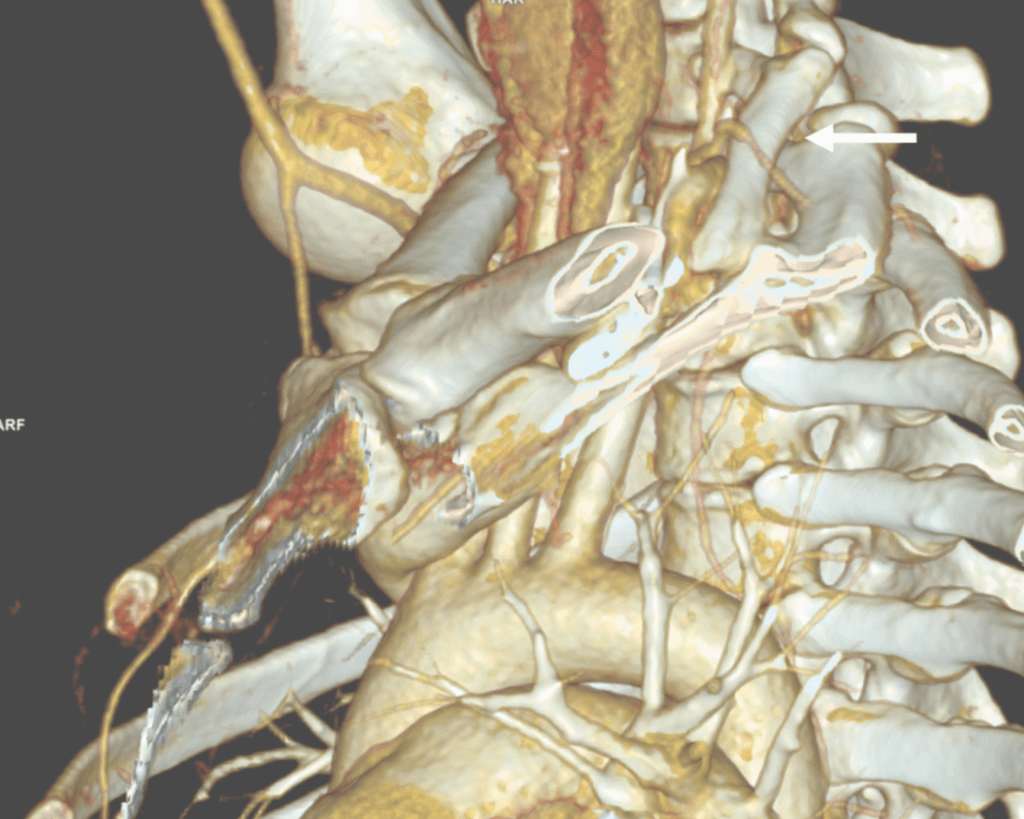
On examination, she was petite and had narrow shoulders. Stress maneuvers extinguished the arterial pulse in both extremities. EAST test was vaguely positive -weakness and numbness in the fingertips. Tapping on the cervical ribs which were prominent bumps in the supraclavicular fossae triggered shooting discomfort in both arms. I ordered a CT scan with contrast -this helps with operative planning as the 3D reconstructions allow you to view the operation before you perform it.
White arrow points to left cervical rib. The artery and plexus which is not seen are draped over it.
I recommended cervical rib resection, bilateral, staged. The left side was chosen first as it was the more symptomatic side. I recruited the assistance of Dr. Nader Habela, our spine surgeon.
Cleveland Clinic Abu Dhabi, has its roots in Cleveland Clinic,and was founded over a century ago in the vasty fields of wartime France by the four founders in an US Army tent. The observation at that time formed the root of the culture, the meme being that without barriers, the distinctions of competitive, siloed specialities made less sense than collective knowledge. It is encapsulated in our words, “To Act As a Unit.” CCAD is close to those roots. Lacking trainees in vascular (working on that), we totally depend on each other for extra pairs of hands in the OR. While it drives my nurses crazy, working with experts in other specialties exposes me to different techniques, instruments, and gadgets, which I load my trays with. Working with Dr. Habela, I saw that for cutting bone in tight spaces, an osteotome and mallet (hammer and chisel) worked with diamond cutter precision is faster and more precise than chewing your way through with a Kerrison. I do wish I had a surgical light saber.
Exposure was via supraclavicular approach. The cervical rib had a joint on the first rib and it was removed. The picture below shows its dimensions.
The artery and brachial plexus were tented up and there was inflammation around these structures. The anterior scalene was released for added measure, but first rib resection, I felt, was unnecessary.
The patient underwent contralateral cervical rib resection a few months later and had significant relief of symptoms but not total relief which I believe has to do with the slower relief time course with neuropathy. The chest pain never recurred. While I do know that diaphragmatic issues refer to the shoulder because of the emryologic origins of the diaphragm and shared roots of the phrenic nerve with brachial plexus, I do not know of a brachial plexus issue referring symptoms to the chest outside of autoimmune neuropathies which the patient did not have. The chest x-ray, which I always get after these procedures to check on diaphragm innervation and for pneumothorax showed the removal of the left cervical rib only, but no insight in why she had chest pain along with the extremity symptoms.
Cervical Ribs Must Go
I have never comes across a benign cervical rib. Because they are easy to remove, they should come out. While no arterial injury had occurred in this patient, we see many instances where compression and aneurysmal degeneration beyond the compression with embolization results in tissue loss, frequently misdiagnosed as rheumatologic arteriopathies. The cervical rib is a special case of neurologic thoracic outlet syndrome (nTOS) where the pathoanatomic mechanism is magnified by the extra bone. While physical therapy has a role in standard nTOS, no amount of PT will address the cervical rib. The inclusion of the Boticelli Venus has to do with the fact that stature and posture plays a significant role in nTOS. Even after first rib resection, there are some people who need a second rib resection to clear the space.
The critical need to treat this is that nerve injury is sometimes irreversible if left untreated. The worst outcome is a causalgia -the feeling that the upper extremity is being electrocuted, put on fire, eaten by flesh eating ants, that is perfectly and completely disabling because our function is defined by our ability to use out upper extremities. Once this sets in, surgical neurolysis or any reoperation has very little chance of working.
So many problems from a bipedal lifestyle
There are so many chronic problems arising from bipedalism, that I will have to work on a whole monograph about it. Humans are the only vertebrates (aside from a few burrowing fish and sea horses) in the history of vertebrates with a vertical spine in orientation to gravity. Yes, there are bipedal dinosaurs like pigeons and velociraptors, but look at their spines -they are horizontal to gravity with the mass centered around the hip. Aside from the obvious ones of spinal compression and arthritis, hernias, and prolapses, are vascular diseases like venous insufficiency, median arcuate ligament syndrome (MALS), and popliteal entrapment. While the first one, venous insufficiency makes sense, MALS does not until you understand how much the heart full of blood weighs. Suspend this bag of meat and blood on your celiac axis, grind the celiac plexus between the diaphragmatic ligaments and the artery, and voila -MALS. Popliteal entrapment -easy – being upright means straightening our knees, something no animal does, which exacerbates the entrapment.
Bonus for my readers -POTS -postural orthostatic tachycardia syndrome -does not exist for quadrupeds -cannot. Our swift (a million years?) transition to bipedalism did not happen with the proper adjustment of our pressure gauges for some, and those with POTS struggle with this change in posture from the natural horizontal state practiced by all other vertebrates.
About ten years ago, I had a patient who came to see me for moderate carotid disease. While his carotid disease was asymptomatic, he also had metastatic colon cancer. With colectomy, cryoablation of liver mets, and chemotherapy, he was in remission. Every 6 to twelve months he had some kind of CT scan with contrast. His renal function was poor and this was blamed on his chemotherapy. While it had nothing to do with this patient, I thought to myself, “Having an aortic stent graft was a lot like having metastatic cancer in remission.” After a stent graft, the patient is forever tied to the health care system. Without surveillance, there may be an endoleak, sac expansion, rupture, and even death. Patients and vascular surgeons can make choices that lengthen life, improve its quality, and avoid the complications of disease. But what if a treatment becomes a condition and a burden on healthcare resources and the patient’s finances?
Fool me once…
Type Ib Endoleak Causing re-Rupture of a previous r-AAA after no surveillance
Take this patient who had previously ruptured his AAA and undergone EVAR. Several years out from his rupture, he ruptured again from a type Ib endoleak due to aneurysmal degeneration of his right common iliac artery. Per his family, he never followed up. Perhaps he assumed he was cured of his disease? Repairing this was tricky, primarily because I hopped up and down, thinking, “I could cure this!” An open revision with a bifurcated graft would eliminate the need for EVAR surveillance, avoid abdominal compartment syndrome, and the physiologic consequences of a large retroperitoneal hematoma. But who wants a laparotomy? Not this patient, who was hypovolemic shock, and whose family chose the minimally invasive option that everyone assumes is better.
Not a clamp
I took him to the hybrid operating room, balloon occluding to stabilize his blood pressure, embolizing the normal internal iliac artery and extending the stent graft into the external iliac artery.
Completion -there is an Amplatzer plug in the right internal iliac artery
This patient stabilized and had abdominal tightness due to his large hematoma which did not need evacuation. After a stay lengthened by concern for abdominal compartment syndrome, moderate pain, fevers, and bilirubinemia (due to the hematoma), he was discharged and never showed up for followup. None of the phone numbers work. Without followup, EVAR is a menace. We will keep trying.
Regrets, I’ve Had a Few…
The great feature of EVAR is that the complications up-front at the time of surgery are wonderfully low. This patient pictured above here presented in middle age with a rupture into the retroperitoneum. He was unconscious and had hemorrhagic shock.
The decision to perform EVAR was made late in the transfer because I did not have the images from the transferring hospital (another subject for another blog post) so I set up for both open repair and EVAR. En route to the OR, I scanned, slowly, through the CT images sent via CD-ROM, and my internal discussion went something like this.
“He’s a 50-something smoker in shock with a contained rupture of a 8cm infrarenal AAA with a good neck. Let’s take care of this in 30 minutes with a percutaneous endovascular aneurysm repair (p-EVAR).”
“He’s a 50-something smoker in shock with a contained rupture with a good neck -let’s take care of this in 90 minutes with a tube graft, open aortic repair (OAR).”
“With p-EVAR, he’s going to have just two groin punctures and much lower complication rate, shorter length of stay, similar to lower mortality. Look -his blood pressure is 75mmHg systolic!“
“That hypotension is permissive to minimize bleeding. With OAR, he’ll avoid abdominal hypertension and complications of a giant hematoma. Because he’s young, he’ll avoid lifelong surveillance. If anyone can clamp this AAA, it’s me...”
“Pride cometh before the fall. Get this man off the table and figure out the logistics later. p-EVAR. You open him up, he’ll exsanguinate and expire before you get the clamp on.“
I sighed, looked up at the gathered team, and announced, “p-EVAR.” The percutaneous EVAR is something I’ve been doing since 2004, long before it was a big deal, and we were done under an hour. His blood pressure stabilized, but general surgery was consulted for his abdominal compartment syndrome. With sedation, fluids and time, his urine out put recovered but his belly remained distended and his bladder pressures which were never seriously elevated, trended down.
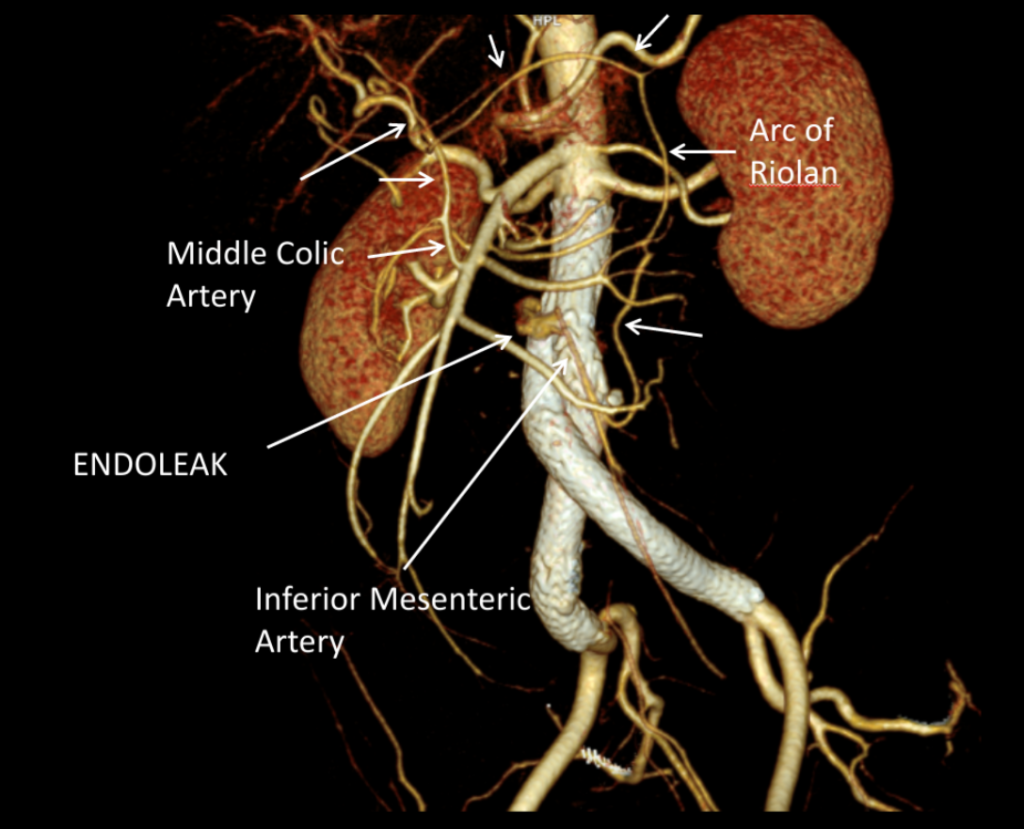
It was made known to me that the patient had very limited insurance making followup surveillance challenging. Due to his coverage, he had to have his imaging done at designated hospitals, so I wrote a detailed note -basically the timings of his followup CT scan, and asked that the reports should be sent to me. I ordered a CTA prior to discharge which showed a type II endoleak adjacent to the graft and connected to both lumbar and inferior mesenteric arteries (first image above). After some thinking, I took the patient for an aortogram, accessed the IMA via the SMA and coiled into his AAA sac and the IMA.
It was only a few weeks ago one of my colleagues across town contacted me that the patient had been admitted with abdominal pain, a CT showing a type II endoleak from his lumbars, but a smaller AAA sac than his pre-repair size of 8.5cm. The patient is seeking to repatriate, and I doubt he would be able to get adequate followup in his home country without paying in cash. Happy that the patient survived his rupture, I still have persistent regrets at not getting him through an open repair, which I am sure he would have done fine with… Or maybe not.
Je Ne Regret Rien…
Recently I admitted a patient, in his 70’s, with a symptomatic 6.5cm infrarenal AAA with bilateral common iliac artery aneurysms, the right being 25mm, the left over 30mm. Because of the pandemic, he was stuck here, seeking to repatriate. Over ten years before, he had a segment of descending thoracic aorta repaired for a traumatic tear -probably one of the last before the wide adoption of thoracic stent grafts which work great by the way.
Cardiac risk evaluation revealed an ejection fraction of 35% with reversible ischemia on nuclear stress test. CTA of the coronaries revealed triple vessel coronary artery disease corroborated by catheterization. Off-pump CABG was planned which would eliminate the effects of cardiopulmonary bypass.
Preparations were made for EVAR with IBE of the left iliac aneurysm as a contingency, but there was no question that if the patient recovered well from his CABG, he would undergo open repair. This was because bell-bottoming or IBE must have regular coordinated surveillance which was not going to be easy with the patient leaving for another country in the middle of a pandemic. It is difficult to get followup to happen in normal circumstances (see above cases). I expressed my opinion to the patient and family and we agreed to see how the patient responded to off-pump CABG.
He underwent off-pump CABG with three vessels revascularized. He was extubated POD#1 and mobilized. By POD #4, he was on a regular patient floor, being co-managed by hospital medicine who takes care of all of our patients. The patient expressed readiness for the next operation. His kidney function remained normal. He was transfused 2 units of PRBC to bring his hematocrit to 30%. He was taken off Plavix, but kept on aspirin. On POD#6, he was taken back to the operating room for open aortic bypass. This would not have been possible without close coordination of cardiology, cardiac surgery, and vascular surgery. Choosing off-pump CABG was a critical element in being able to proceed with open aortic surgery.
Right branch taken to iliac bifurcation, separate bypasses sent to left internal and external iliac bypasses.
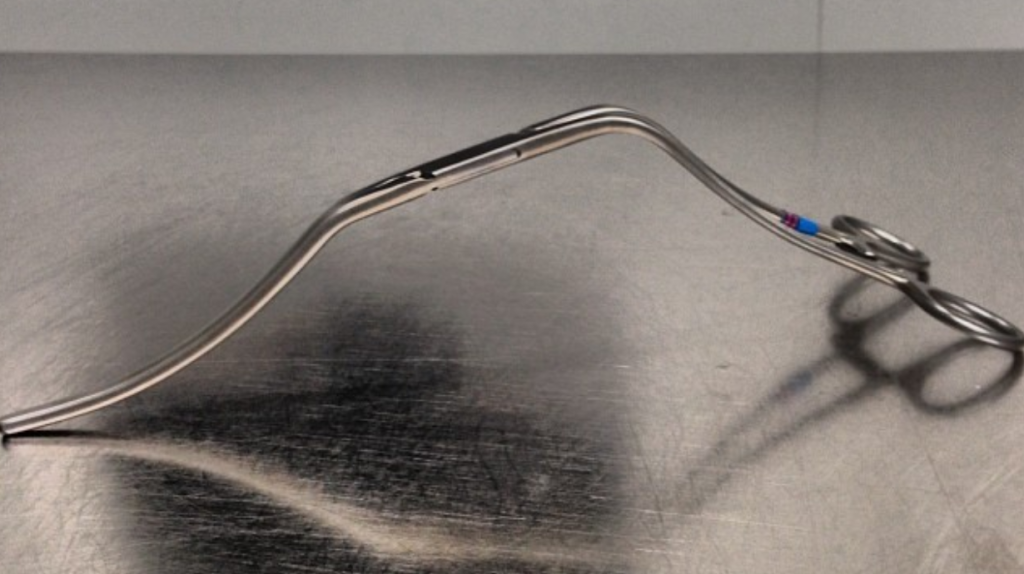
I do several things to decrease the physiologic impact of the operation. First is keeping all the viscera retracted under the skin. This simple move has the effect of decreasing the rate of intestinal paralysis and amount of fluid shifts that occur postop, akin to going retroperitoneal. This decreases the space you potentially have if you use standard clamps, but I use the Cherry Supraceliac clamp (image), DeBakey Sidewinder (transverse), or just a Satinsky clamp oriented transversely. This minimizes the occupation of volume over the anastomosis which always happens with standard aortic cross clamps. The anastomosis is easier without the clamp taking up valuable space.
Cherry Supraceliac Aortic Clamp
The iliacs are always clamped with Wylie Hypogastric clamps, again, with the principle of eliminating clamp overhang. Suturing is done with 4-0 Prolene on SH needles -this is plenty (link). The proximal anastomosis wants to bleed, and sewing to a fully cut ring of aorta ensures good posterior bites but also allows for sliding a band of graft down over the anastomosis (Dan Clair calls this a gusset) which works well at creating a hemostatic proximal anastomosis rapidly-trust me, getting this done well is the key step of the operation. Before closing, I infiltrate the rectus sheath and preperitoneum bilaterally with local anesthesia -lidocaine 1% with epinephrine 1:1 with bupivicaine 0.5%. The skin is closed with absorbable dermal sutures because staples create as many problems as they solve. The patient had cell salvage through the case and no extra units of transfused blood.
The patient was extubated that night and started on clear liquid diet. The next day his lines were removed and he was moved to the floor and started on regular diet when he expressed hunger. On POD#2, he was pacing floor, asking when he could be discharged.
Sternotomy and Laparotomy POD#2, walking the floor
As he was eating, walking, talking, breathing, evacuating bowel and urine, and pain free (well controlled), I saw no reason to keep him beyond POD #3 AAA/#9 CABG. I have kept in touch with him and his family and he is doing well and has given permission for this posting.
Satisfaction
This final case has confirmed several of my beliefs. First, calling something high risk can drive one to make bad choices and in fact endanger patients. This last patient would qualify as high risk on any international criteria, and you would not be wrong in quoting upwards of 30% major morbidity and mortality for cardiac revascularization and AAA repair, but you would also be tying your hands from offering the best solution for this man who fortunately was able to undergo two prodigious operations. He will not require much in the way of followup. Coronary revascularization with arterial conduit and open aortic grafting frees him from the need for close followup and reassures us that his repair is durable.
Second, calling something advanced and minimally invasive gives one cachet in the marketplace but forgoes careful discussion and consideration of what is being abandoned. The first two patients survived their ruptures but now face the consequences of having stent grafts. It is a shame when podium speakers at international symposia declare surgery to represent failure because this affects training by encouraging abandonment of hard to acquire skills. It seeps into patient perceptions and expectations. I hope that a balanced approach prevails. You have to be capable of both open and endovascular approaches to be able to offer the best treatment for a particular patient.
Finally, these old operations are cost efficient and there is a lot of room to improve these procedures with new perspectives, techniques, and data. I don’t operate the same way I trained, and it is only through continued application of operations that improvements can come about. As budgets tighten and economies are stressed, cost efficacy will rein in much of the interest and demand in new stuff unless it adds value. That said, I am grateful to our stent graft representatives who have worked to get us bell bottoms and IBE’s for when they will be needed. These grafts will be used when the time is right.