

When Australopithecus began to walk upright, there were many consequences. It freed the hands from weight bearing, but it also burdened the shoulder girdle with the weight of the extremity. Boticelli’s Venus shows the Renaissance ideal of the narrow shouldered maiden, but that bulk of shoulder and arm meat and bone, roughly equal to the weight of a jamón ibérico (vacation pic below), hangs off the neck with pathologic consequences. Also, the australopithecine usually died by disease or trauma by the second decade if chimpanzees are to be believed, but we live for nearly a century wearing down tissues designed for 10-20 years.

Mechanically speaking, there is a weight and a rope. The brachial plexus is the rope and it is draped over the first rib. The muscles of the shoulder girdle should support the weight of the arm but with bad posture, another consequence of bipedalism, the muscles may not be up to the task.

When there is a cervical rib, the situation is worse. The thoracic outlet is narrowed, and the weight of the arm, the jamón, is borne on the cervical rib. The brachial plexus becomes stretched over this anomalous bone and the trauma results in symptoms of pain, weakness, and strange sensations. I am of the opinion that cervical ribs in general should just go when found as nerve (and arterial) injury when found late may be irreversible.
CASE
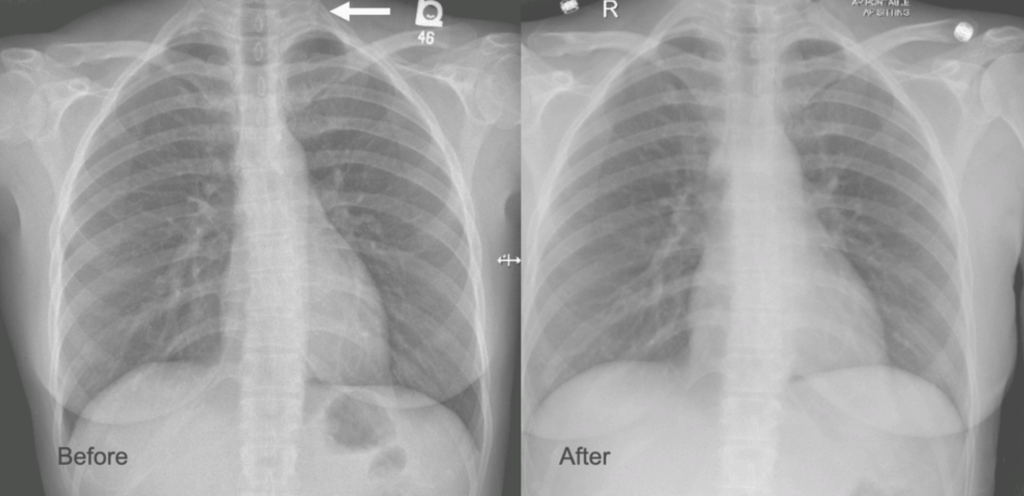
The patient is a younger woman who was referred from cardiology after workup of chest pain and left arm pain was negative for cardiac disease. She also had occasional right arm pain. The only finding of note during an extensive cardiac workup were cervical ribs found bilaterally on chest x-ray (below).

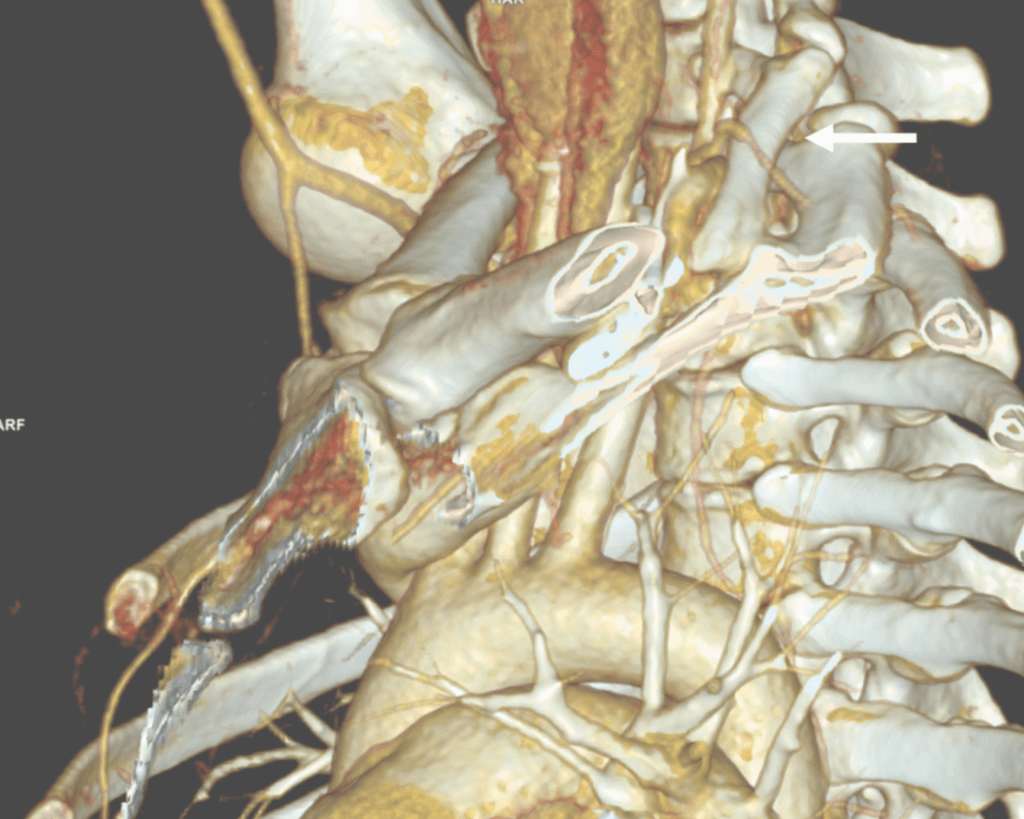
On examination, she was petite and had narrow shoulders. Stress maneuvers extinguished the arterial pulse in both extremities. EAST test was vaguely positive -weakness and numbness in the fingertips. Tapping on the cervical ribs which were prominent bumps in the supraclavicular fossae triggered shooting discomfort in both arms. I ordered a CT scan with contrast -this helps with operative planning as the 3D reconstructions allow you to view the operation before you perform it.

I recommended cervical rib resection, bilateral, staged. The left side was chosen first as it was the more symptomatic side. I recruited the assistance of Dr. Nader Habela, our spine surgeon.
Cleveland Clinic Abu Dhabi, has its roots in Cleveland Clinic,and was founded over a century ago in the vasty fields of wartime France by the four founders in an US Army tent. The observation at that time formed the root of the culture, the meme being that without barriers, the distinctions of competitive, siloed specialities made less sense than collective knowledge. It is encapsulated in our words, “To Act As a Unit.” CCAD is close to those roots. Lacking trainees in vascular (working on that), we totally depend on each other for extra pairs of hands in the OR. While it drives my nurses crazy, working with experts in other specialties exposes me to different techniques, instruments, and gadgets, which I load my trays with. Working with Dr. Habela, I saw that for cutting bone in tight spaces, an osteotome and mallet (hammer and chisel) worked with diamond cutter precision is faster and more precise than chewing your way through with a Kerrison. I do wish I had a surgical light saber.

Exposure was via supraclavicular approach. The cervical rib had a joint on the first rib and it was removed. The picture below shows its dimensions.

The artery and brachial plexus were tented up and there was inflammation around these structures. The anterior scalene was released for added measure, but first rib resection, I felt, was unnecessary.
The patient underwent contralateral cervical rib resection a few months later and had significant relief of symptoms but not total relief which I believe has to do with the slower relief time course with neuropathy. The chest pain never recurred. While I do know that diaphragmatic issues refer to the shoulder because of the emryologic origins of the diaphragm and shared roots of the phrenic nerve with brachial plexus, I do not know of a brachial plexus issue referring symptoms to the chest outside of autoimmune neuropathies which the patient did not have. The chest x-ray, which I always get after these procedures to check on diaphragm innervation and for pneumothorax showed the removal of the left cervical rib only, but no insight in why she had chest pain along with the extremity symptoms.
Cervical Ribs Must Go
I have never comes across a benign cervical rib. Because they are easy to remove, they should come out. While no arterial injury had occurred in this patient, we see many instances where compression and aneurysmal degeneration beyond the compression with embolization results in tissue loss, frequently misdiagnosed as rheumatologic arteriopathies. The cervical rib is a special case of neurologic thoracic outlet syndrome (nTOS) where the pathoanatomic mechanism is magnified by the extra bone. While physical therapy has a role in standard nTOS, no amount of PT will address the cervical rib. The inclusion of the Boticelli Venus has to do with the fact that stature and posture plays a significant role in nTOS. Even after first rib resection, there are some people who need a second rib resection to clear the space.
The critical need to treat this is that nerve injury is sometimes irreversible if left untreated. The worst outcome is a causalgia -the feeling that the upper extremity is being electrocuted, put on fire, eaten by flesh eating ants, that is perfectly and completely disabling because our function is defined by our ability to use out upper extremities. Once this sets in, surgical neurolysis or any reoperation has very little chance of working.
So many problems from a bipedal lifestyle
There are so many chronic problems arising from bipedalism, that I will have to work on a whole monograph about it. Humans are the only vertebrates (aside from a few burrowing fish and sea horses) in the history of vertebrates with a vertical spine in orientation to gravity. Yes, there are bipedal dinosaurs like pigeons and velociraptors, but look at their spines -they are horizontal to gravity with the mass centered around the hip. Aside from the obvious ones of spinal compression and arthritis, hernias, and prolapses, are vascular diseases like venous insufficiency, median arcuate ligament syndrome (MALS), and popliteal entrapment. While the first one, venous insufficiency makes sense, MALS does not until you understand how much the heart full of blood weighs. Suspend this bag of meat and blood on your celiac axis, grind the celiac plexus between the diaphragmatic ligaments and the artery, and voila -MALS. Popliteal entrapment -easy – being upright means straightening our knees, something no animal does, which exacerbates the entrapment.
Bonus for my readers -POTS -postural orthostatic tachycardia syndrome -does not exist for quadrupeds -cannot. Our swift (a million years?) transition to bipedalism did not happen with the proper adjustment of our pressure gauges for some, and those with POTS struggle with this change in posture from the natural horizontal state practiced by all other vertebrates.


One reply on “Our Bipedal Lifestyle Has Consequences, or Cervical Ribs Must Go”
Hello Dr. Park,
I came across your article and couldn’t help but ask you for a consultation, hoping that this doesn’t bother you.
I’m 24 years old with chronic middle to upper back pain, x-rays and MRIs are normal and unfortunately I couldn’t get a real reason for the pain after going to several doctors.
My back muscles are always stiff no matter how much PT I had or stretching excersises I make, even my chest makes cracking noise when I stretch.
I’ve two cervical ribs so I’m wondering if they somehow could be the reason? and how to test for that?
Thank you very much.
LikeLike