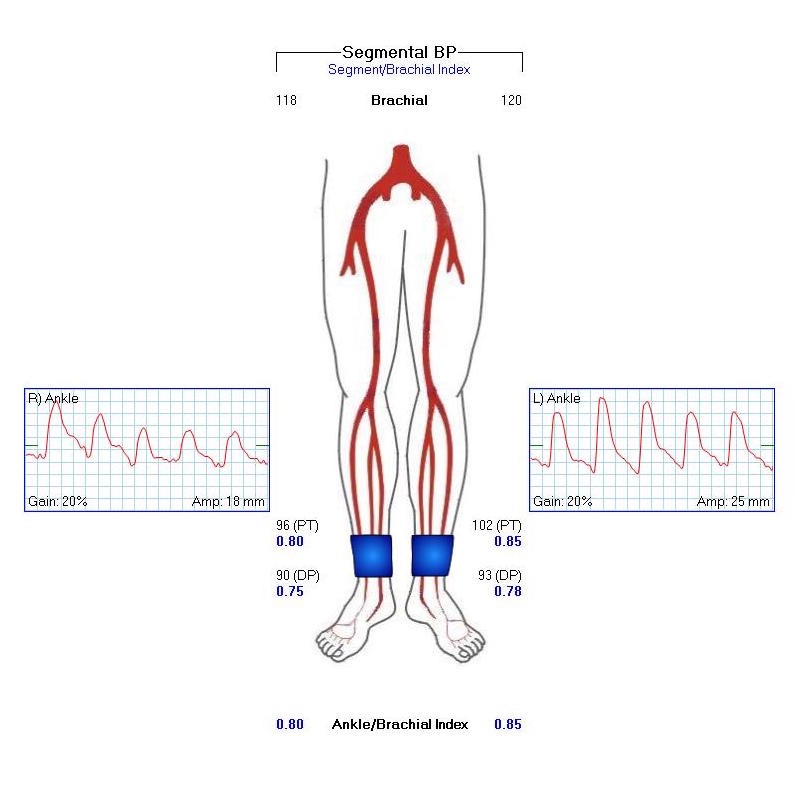
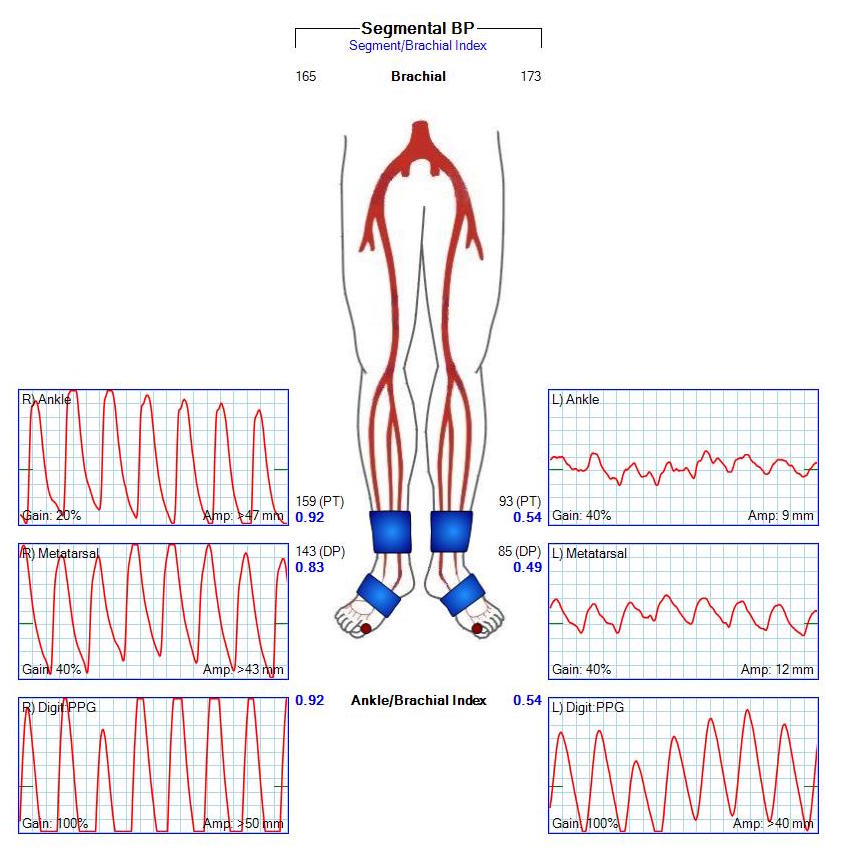
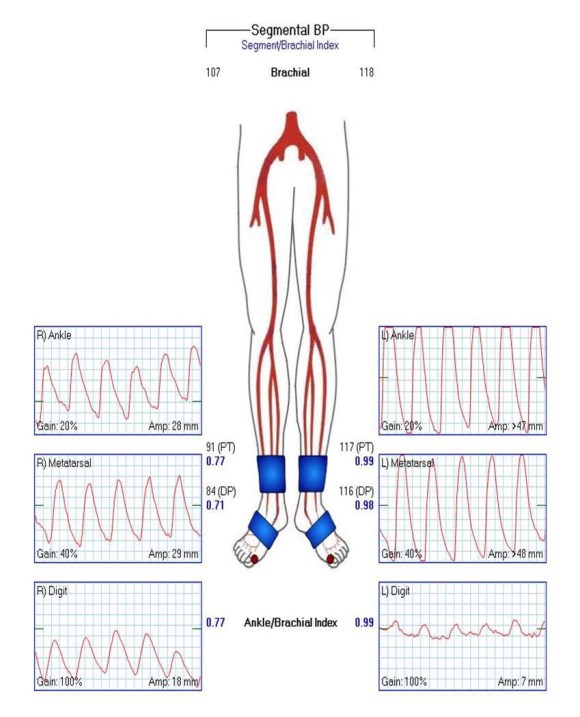
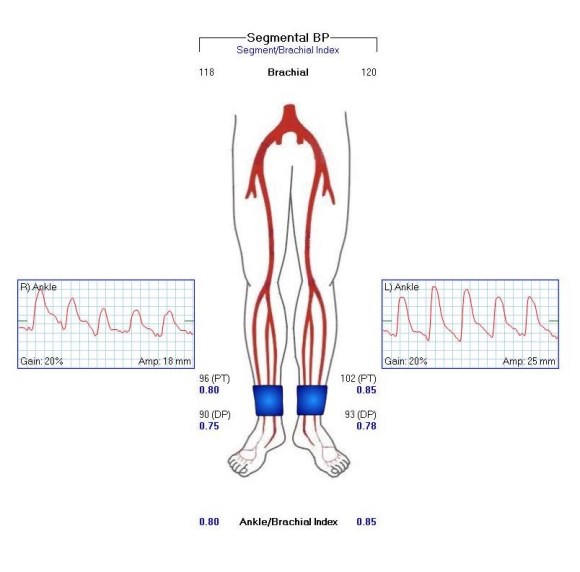
The patient is 70 year old woman with prior history of smoking who developed severe claudication and near rest pain. She was unable to walk more than 50 feet before having to stop due to severe leg pain. On exam, neither femoral artery pulses were palpable. PVR’s (pulse volume recordings) and ABI’s (ankle brachial index) are shown below.

PVR’s demonstrate the presence of severe inflow (aortoiliac occlusive disease or AIOD). CTA was acquired and the findings were consistent with the PVR’s.

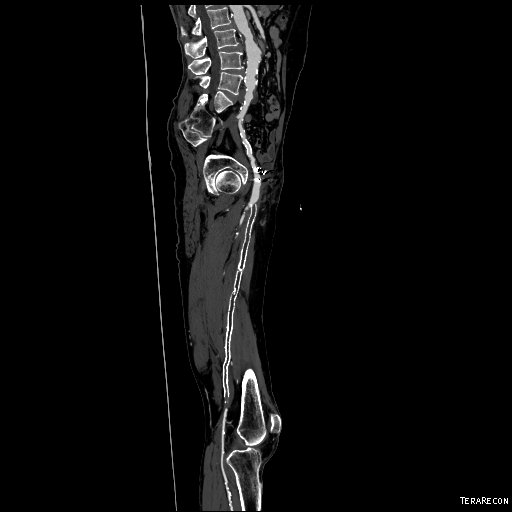
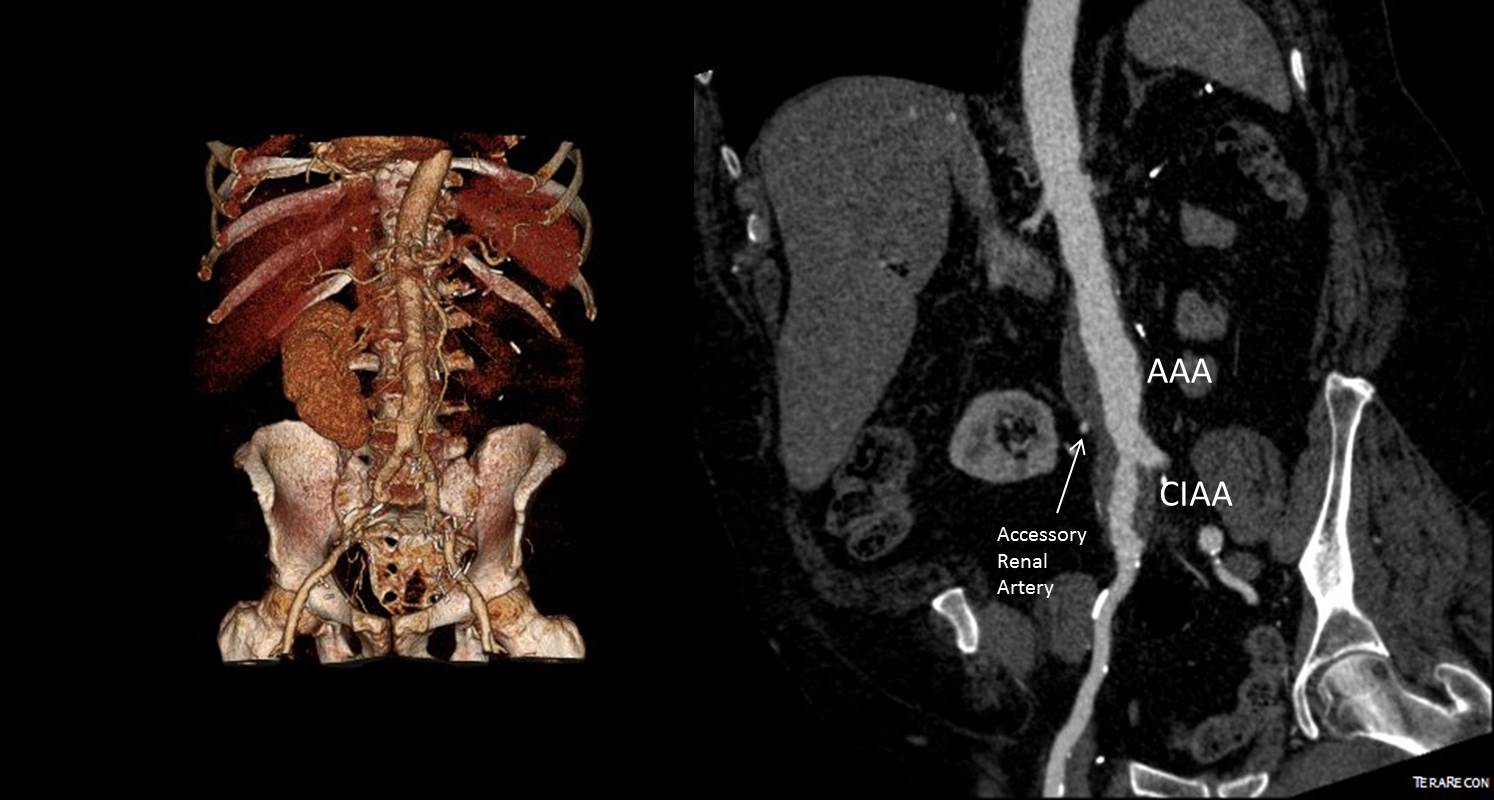
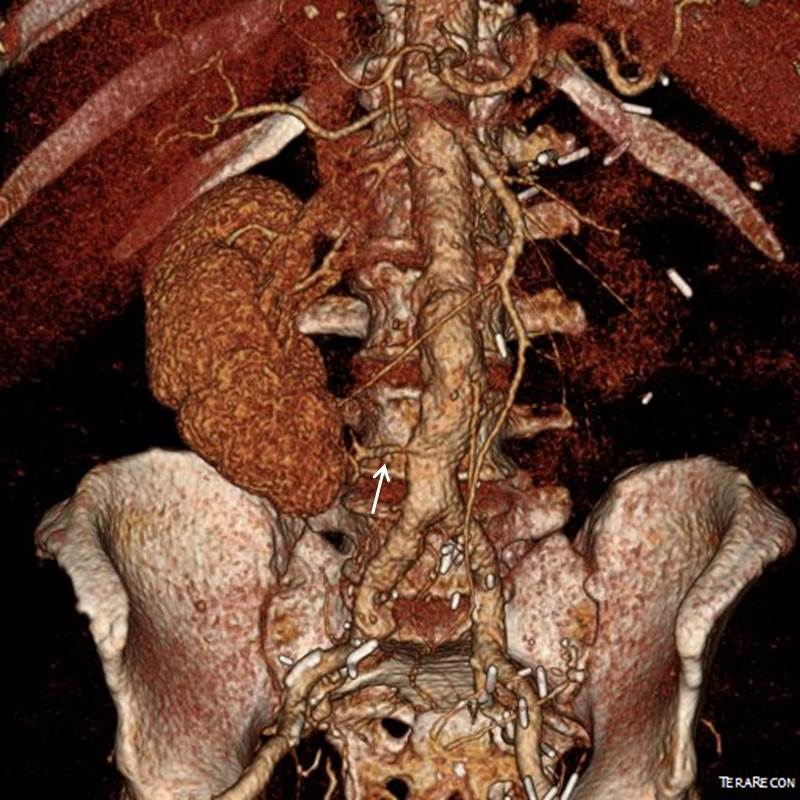
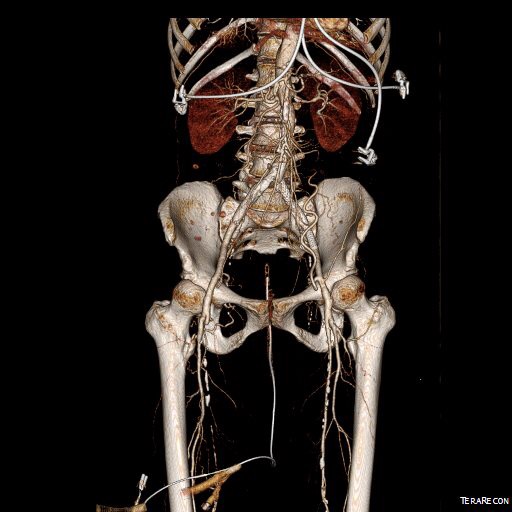
There was diffuse bilateral iliac atherosclerotic plaque with occlusion of the right common femoral artery and left common and external iliac artery. The 3DVR (three dimensional virtual reality) reconstruction image below shows this as well as the abdominal and pelvic wall collaterals feeding the legs around the occluded iliofemoral system.

Plans were made to perform a hybrid common femoral and profunda femoral endarterectomy, remote external iliac artery endarterectomy (EndoRE), and common iliac artery stenting. The specific challenges to this case was getting into and staying in the true lumen. Typically, this is easiest to achieve from a left arm access with wires being pushed antegrade, but in a smaller person, particularly woman, this increases the chances for access site complications. My plan was to expose both common femoral arteries and get control of the external iliac arteries at the inguinal ligament and the profunda femoral arteries at the point the proximal plaque dissipated -typically at the second branch point, and then get micropuncture access of the right iliac system by accessing from the common femoral plaque. This would give me true lumen access, and with a sheath and curved catheter (VCF in this case, but a similarly shaped OMNI Flush catheter would do as well), wire access up and across the occluded left iliac system could be achieved and the wire retrieved from the left common femoral artery. This up and over access with the wire allows for control of the aortic bifurcation and both iliac systems.
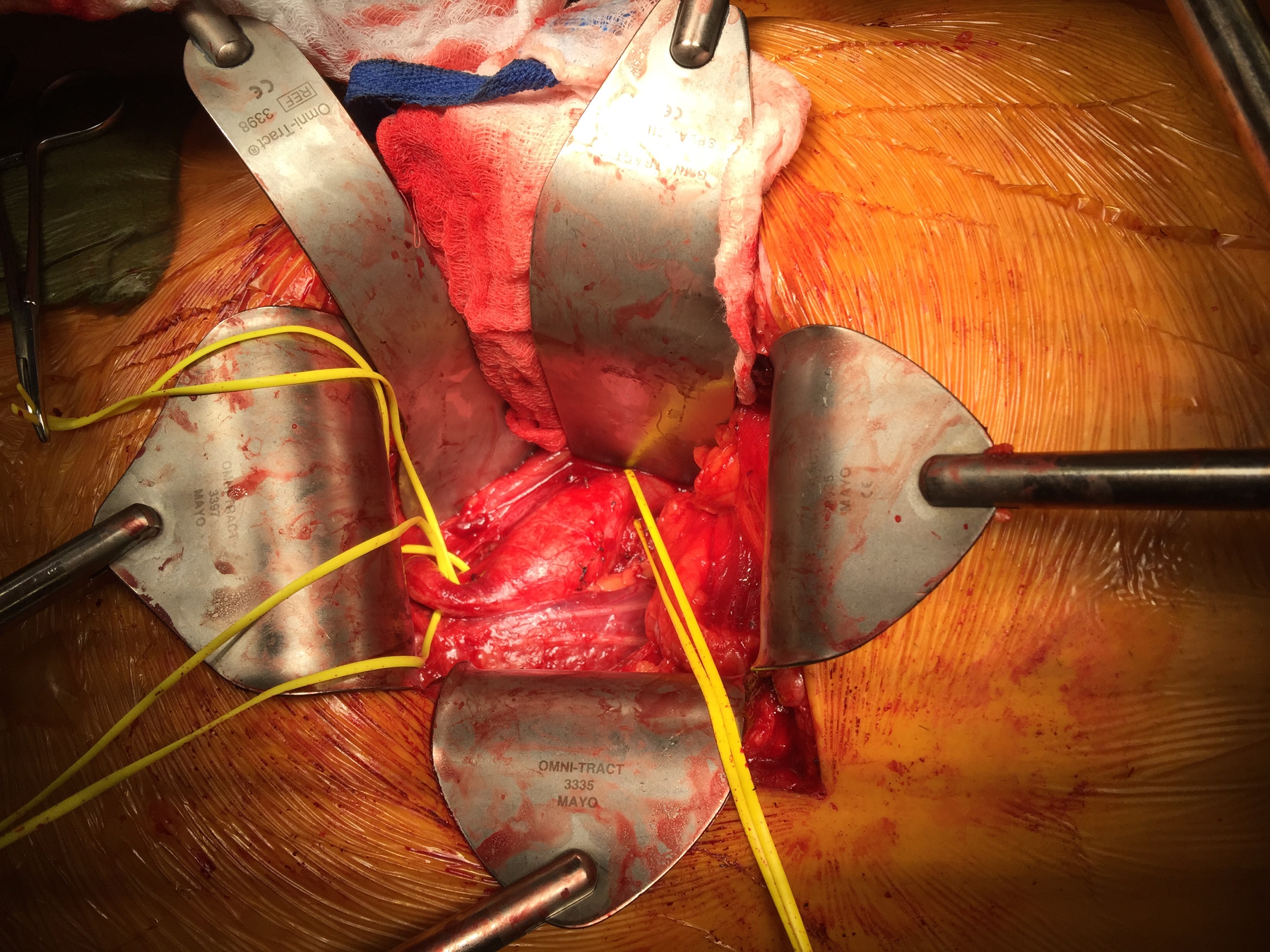
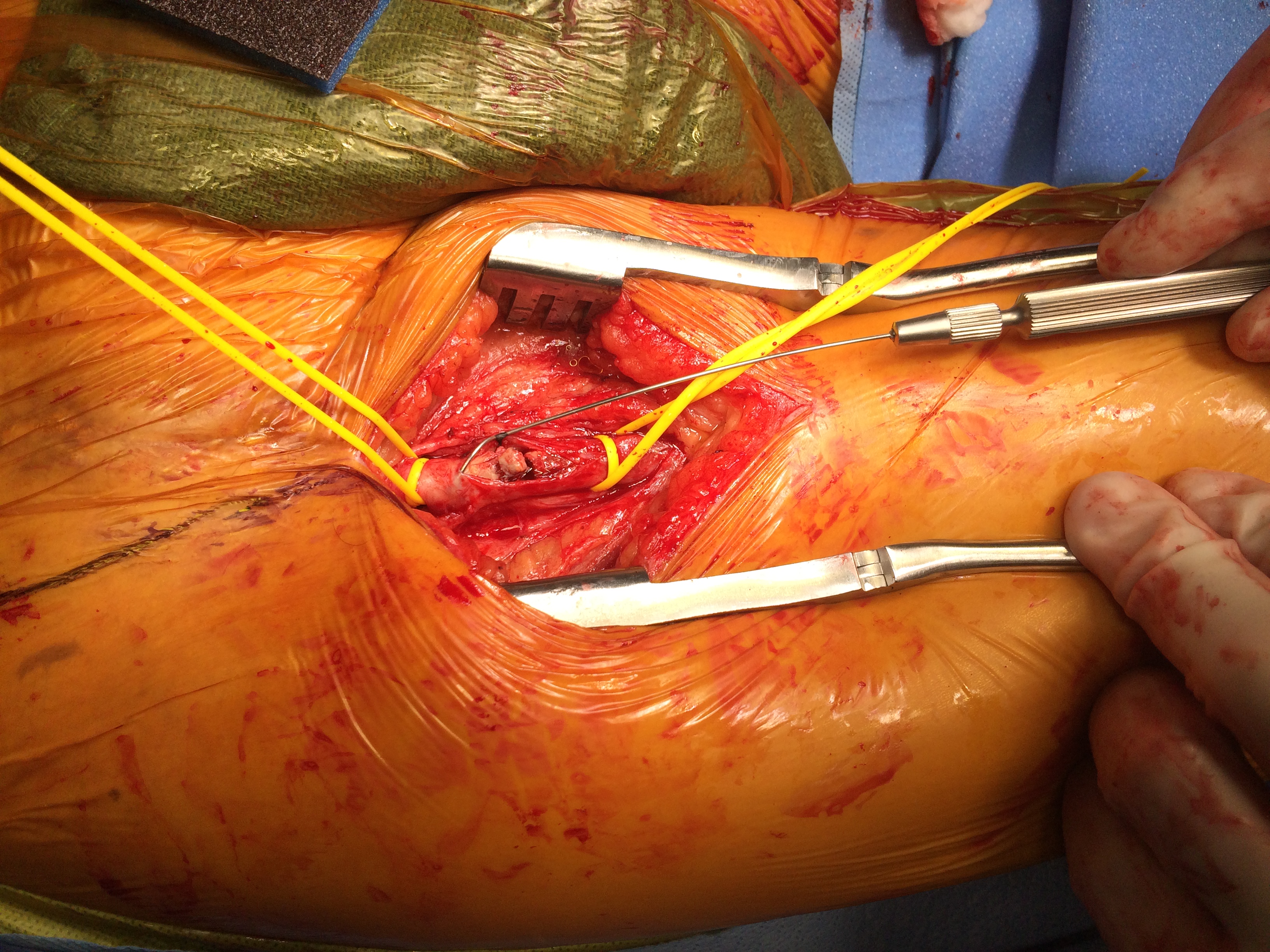
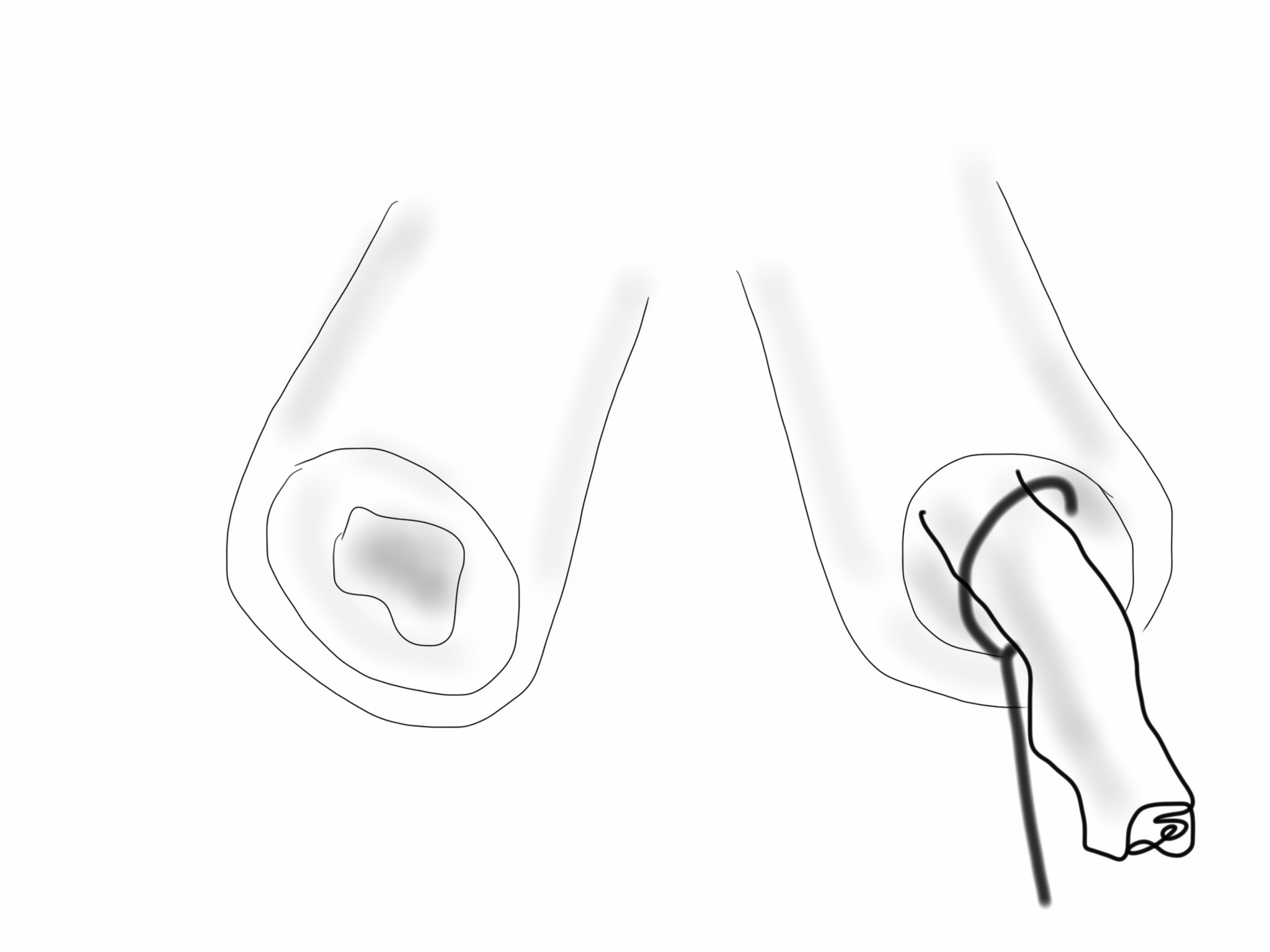
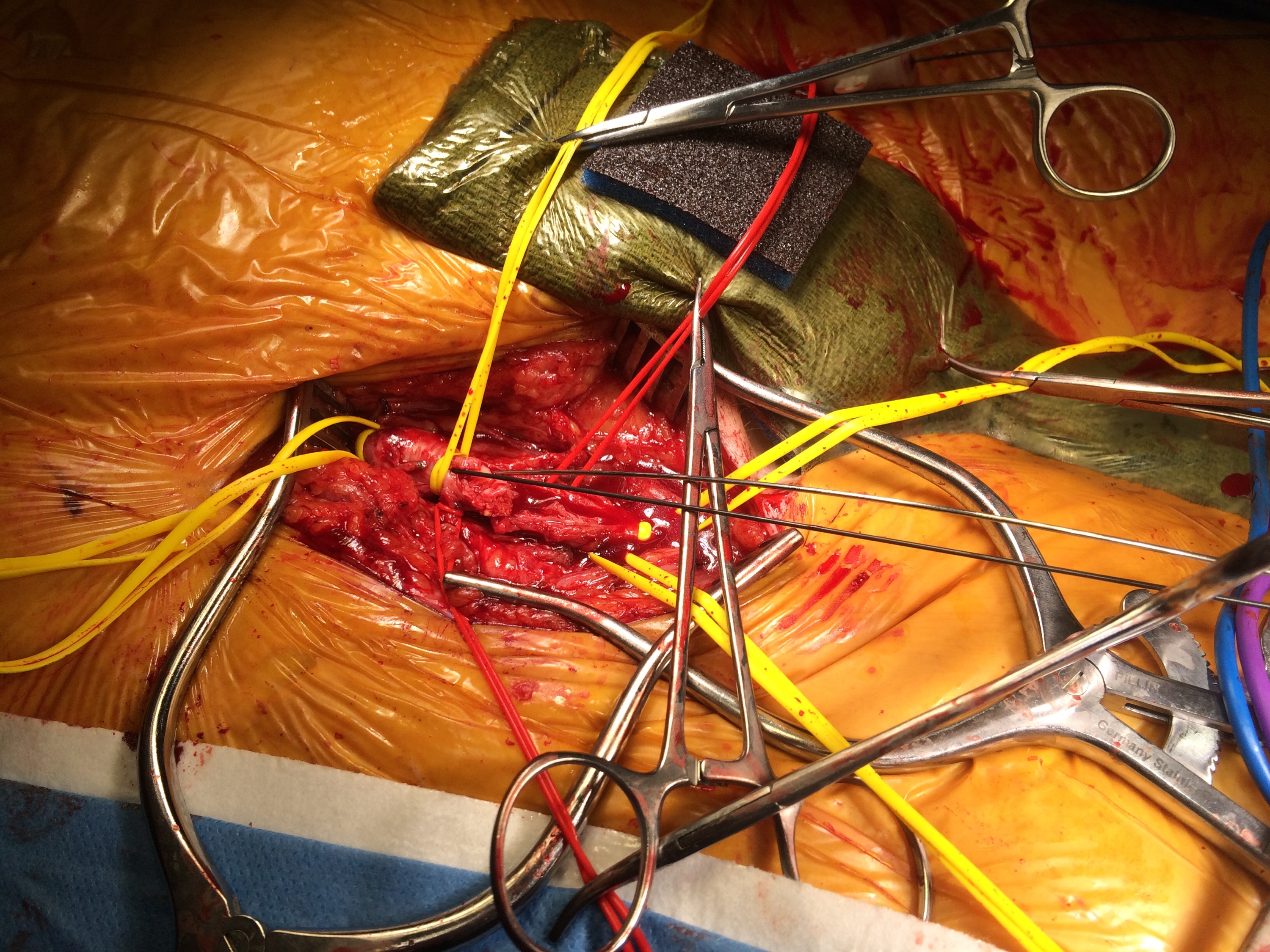
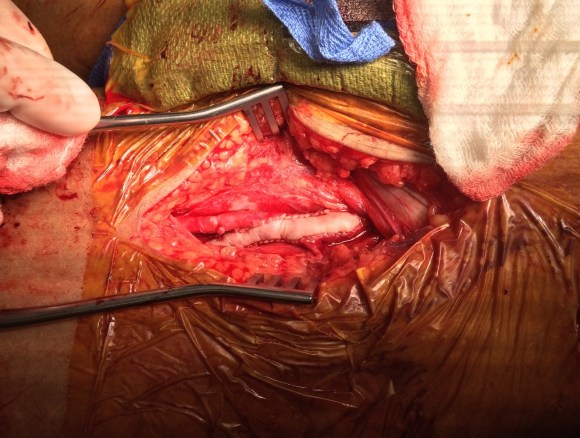
I perform EndoRE over this wire -this allows for quick access if the artery is ruptured. To minimize blood loss, I gain control of the common femoral artery in the following fashion -a 4cm segment of common femoral artery is left intact and looped above the inferior epigastrics -this loop is brought out in the lateral lower quadrant of the abdomen so that the loop doesn’t travel distally over the arteriotomy. The second loop adjacent to the arteriotomy is sent through periadventitial tissues behind the artery to keep the loop migrating over the arteriotomy. The arteriotomy is created from the distal CFA (common femoral artery) onto the profunda femoral artery (PFA) where the endarterectomy is started. A separate arteriotomy on the superficial femoral artery (SFA) allows me to divide the plaque and mobilize the proximal segment up to the SFA origin, freeing the CFA plaque in this manner. It also gives me the option to perform EndoRE of the SFA if warranted. The dissected plaque and system of loops which I call the blood lock is shown below:

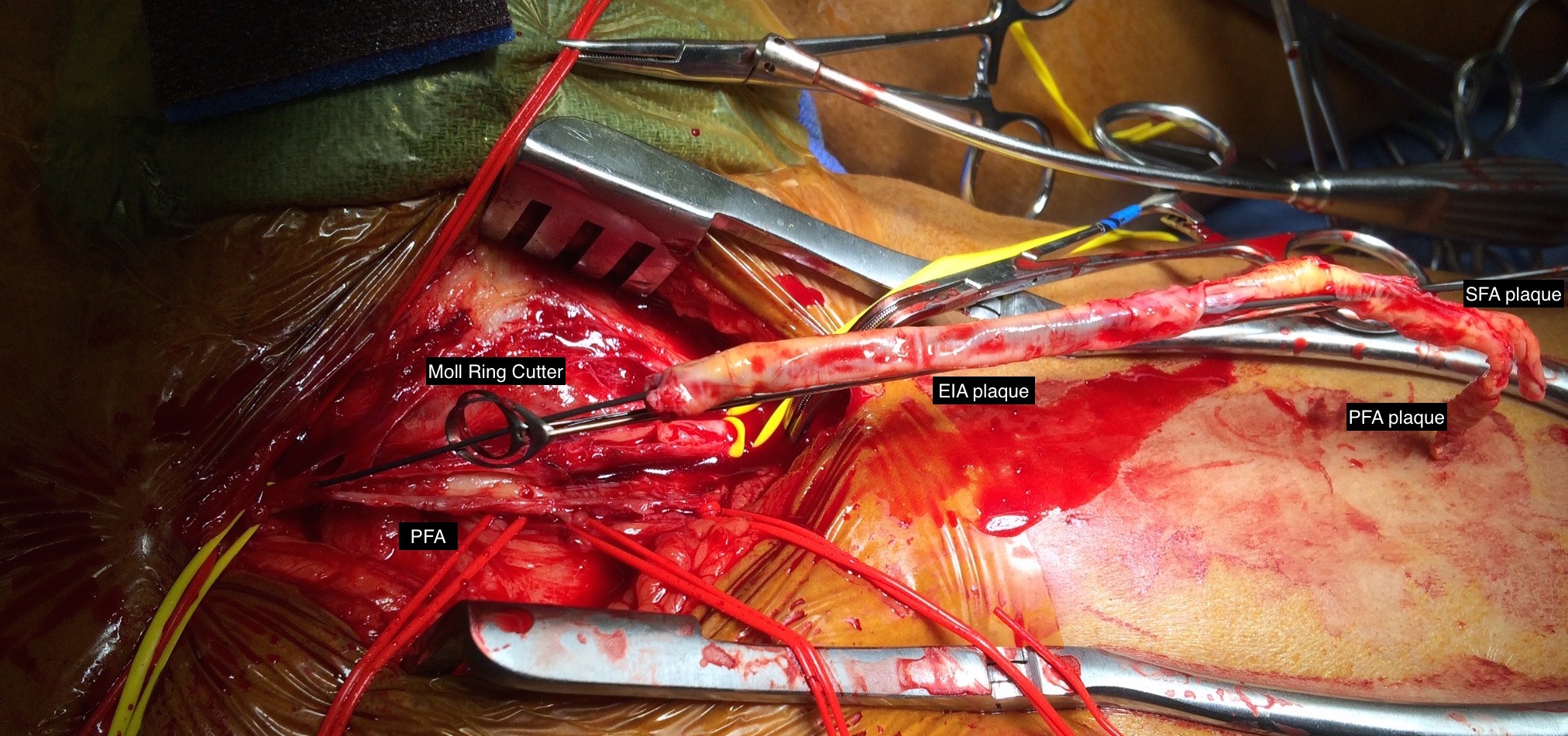
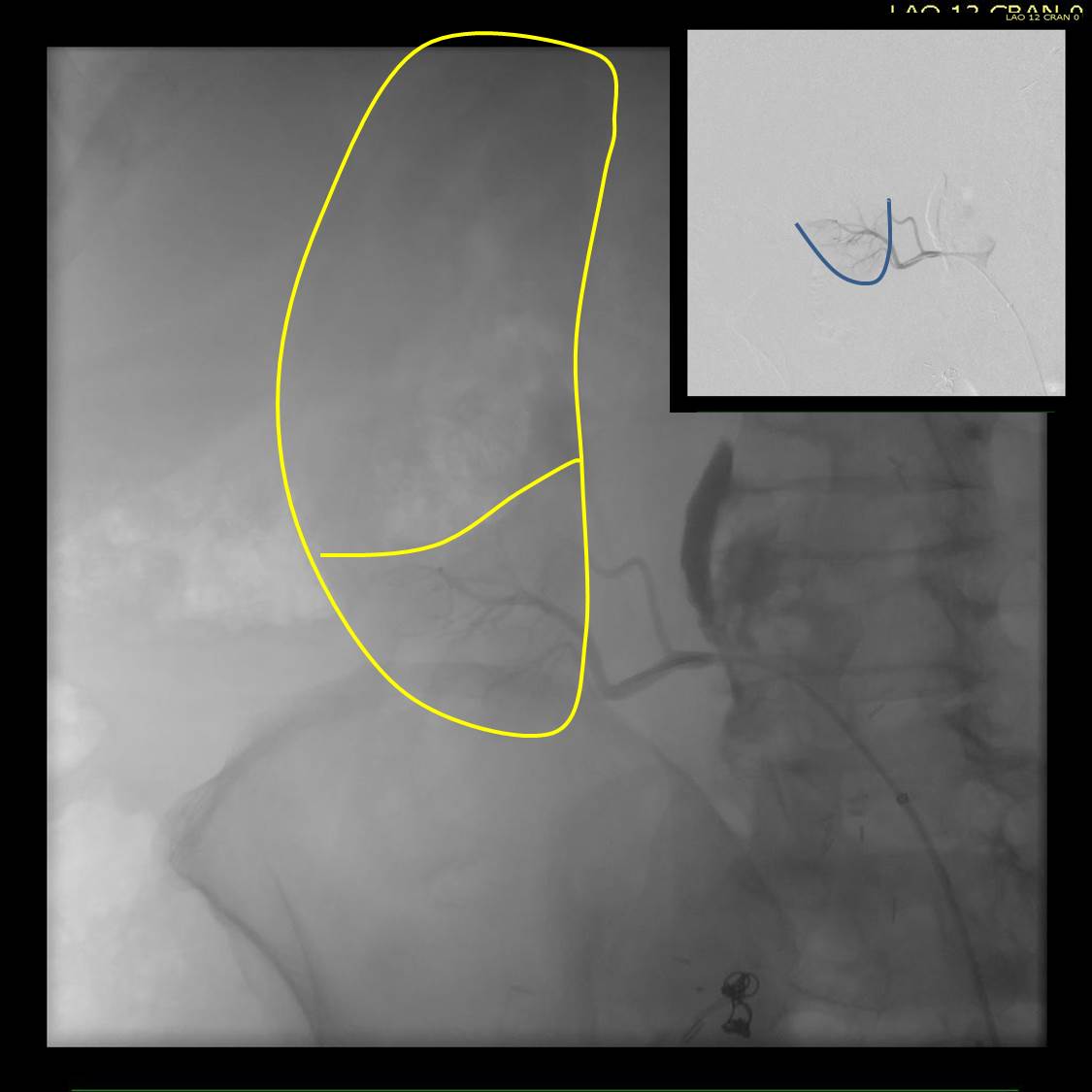
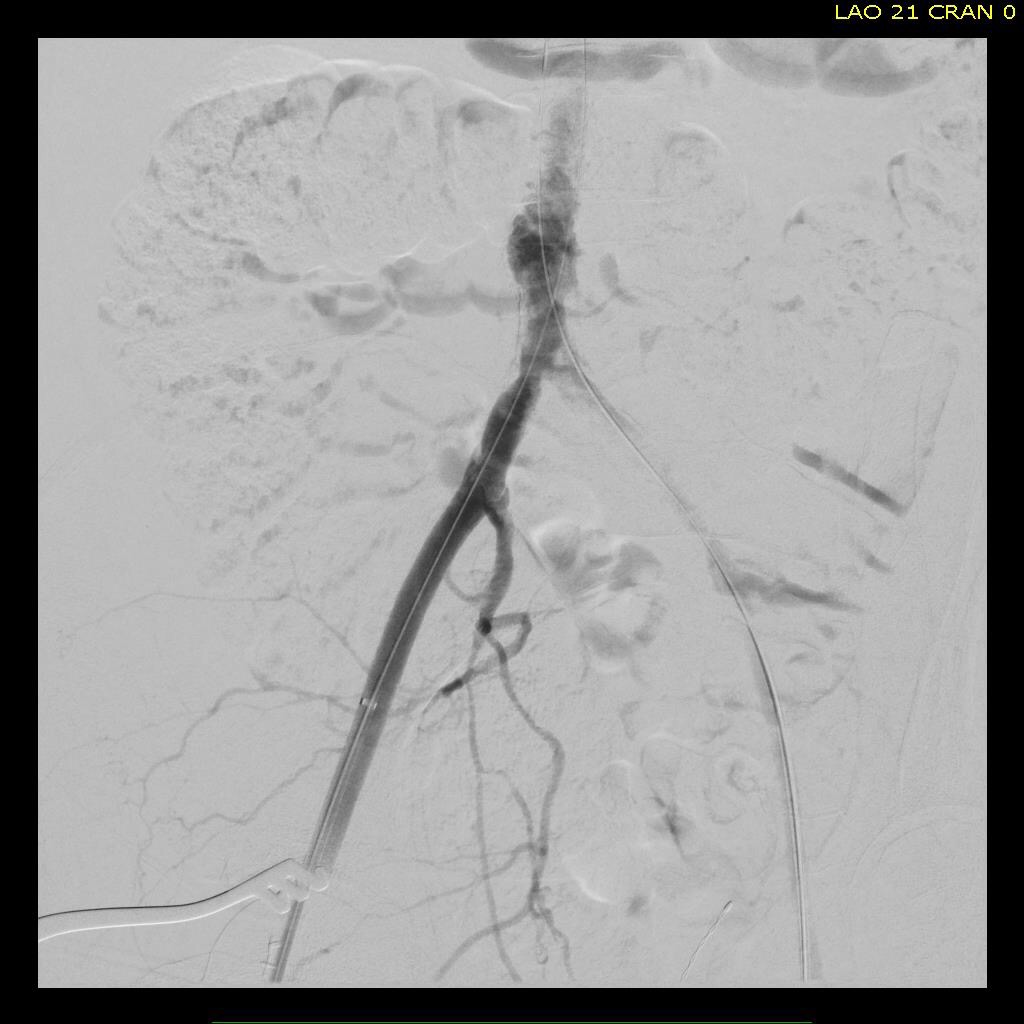
The yellow loops are major control points (the blood lock loop is drawn in the picture above) and the red loops are around smaller branch arteries. At this point, micropuncture access through the plaque core was achieved into the true lumen of the yet patent EIA (external iliac artery, picture below).

The right EIA plaque was mobilized with a Vollmer ring dissector, and cut with a Moll ring cutter (LeMaitre).

This allowed for cutting and removal of the plaque.

Up and over access and control of the wire from the contralateral (left) arteriotomy allowed for EndoRE on the other side. The occluded left common iliac plaque was ballooned and wire access into the aorta from the left was achieved.

Kissing balloon angioplasty was performed with revascularization of the aortoiliac bifurcation and common iliac arteries.

The stents were extended across the dissected end points of the external iliac artery origins. The arteriotomies were closed with bovine pericardial patches. Because the PFA were of small caliber, to avoid narrowing the distal end of the patch, the patches were sewn over Argyll shunts which also allowed perfusion of the legs during the suturing of the patches. The loops made this a straighforward maneuver.
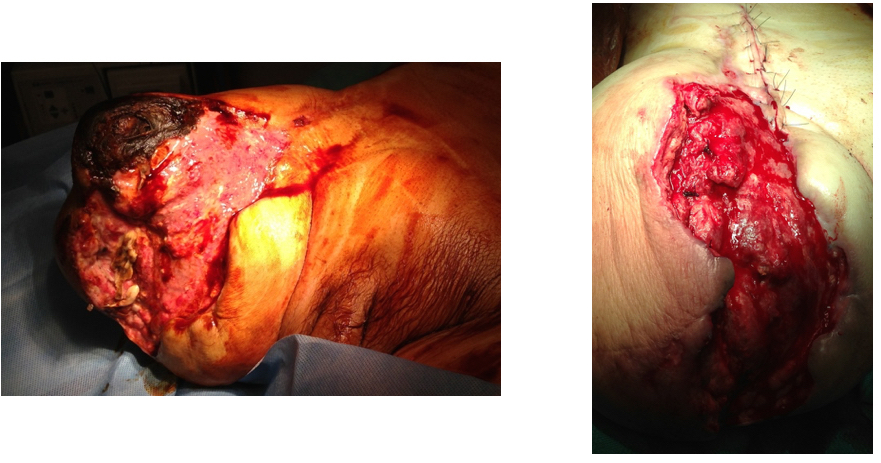
The completed CFA to PFA patch on the left is shown below:
Closure involved reapproximating the Scarpa’s type investing fascia of the femoral triangle and a running dermal layer of absorbable monofilament, dressed with a surgical glue. No drains were used, but if needed, they would be exited through the counter incisions created for the EIA loops.
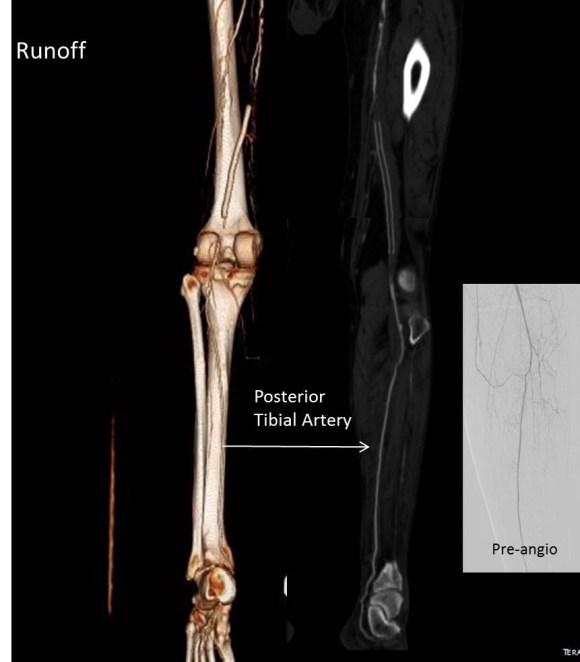
The patient recovered well. I always use cell salvage -sometimes, profundaplasties can be bloody, particularly if they are in reoperative fields. The ABI’s and PVR’s at the ankles improved significantly.
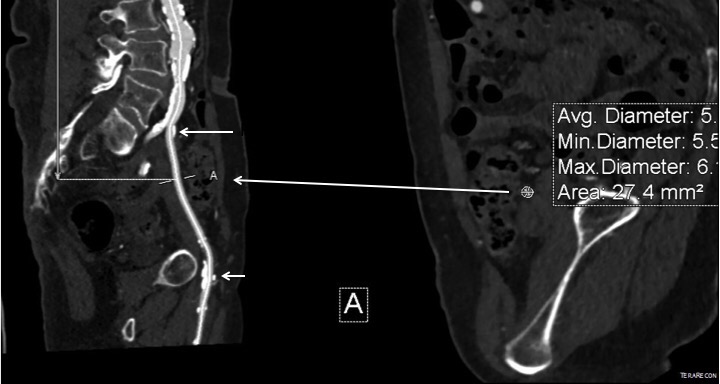
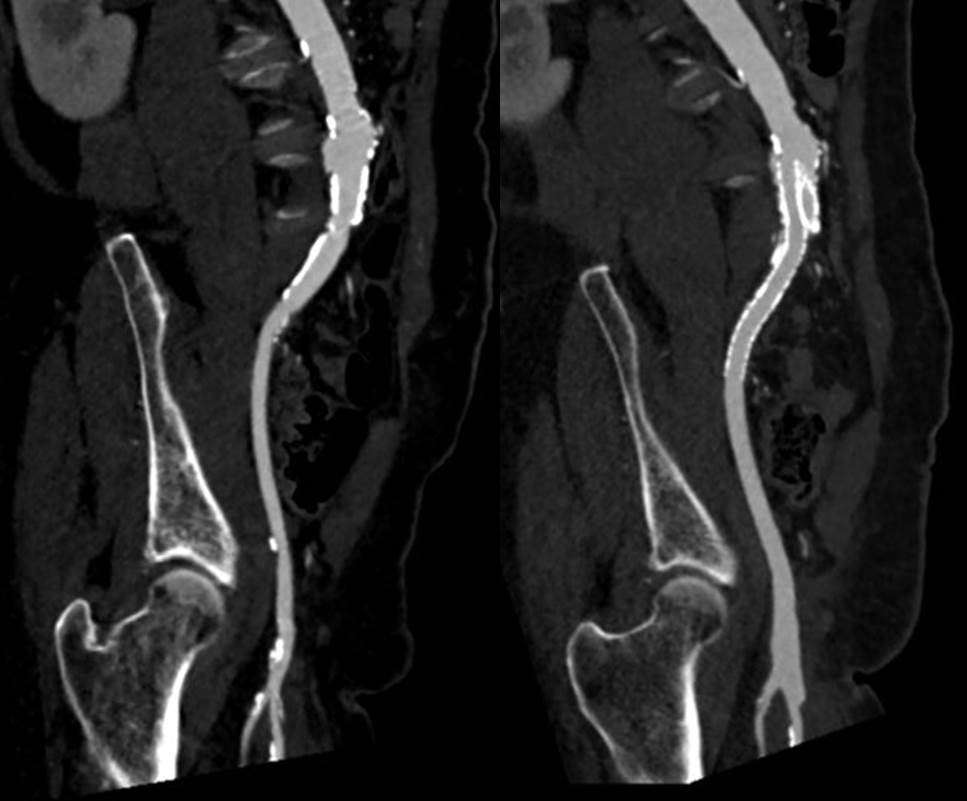
 The postoperative CTA shows good results as well. Below is the composite right and left centerline from aorta to the PFA’s.
The postoperative CTA shows good results as well. Below is the composite right and left centerline from aorta to the PFA’s.

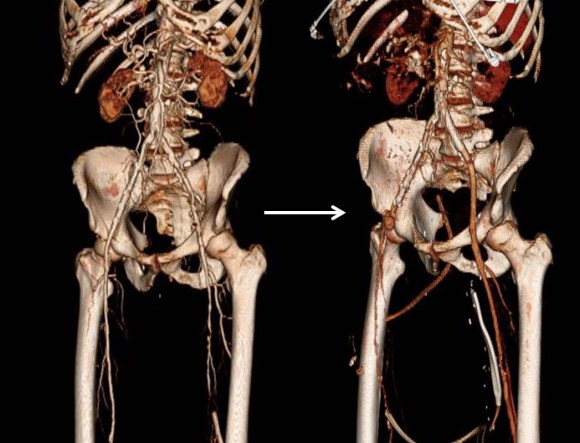
The 3DVR reconstruction images are shown below, with the comparison to preop shown in the first image of this blog entry:
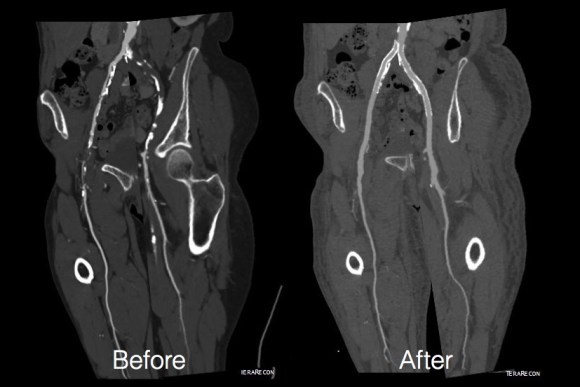
The pre and postoperative images of the centerlines (composited) are shown below:
EndoABF is an established hybrid procedure involving an open endarterectomy of the common femoral and PFA/SFA with iliac balloon angioplasty and stenting, often taking the stents distally into the CFA and the patch to deal with complex distal EIA plaque. This procedure, which would be an EndoRE ABF, offers some advantages in eliminating the need for EIA stents which are often placed across the inguinal ligament and into the patch during EndoABF. In my experience, the EIA EndoRE performed as an extension of a CFA endarterectomy is safe, and made even safer by performing the EndoRE over a wire. Published results from Europe shows for TASC C and D disease, EIA EndoRE has excellent patency, and I would expect the same here. EndoRE and Endo ABF both offer advantages over traditional ABF, particularly in patients with medical comorbidities.