

The patient had an isolated 3.0cm common iliac artery aneurysm. Patient is in his fifties and wants to avoid the need for annual CT scans, buttock claudication. He had also read about neurological complications with open aortic surgery like retrograde ejaculation.
An older patient may be well served with hypogastric artery embolization and iliac stent grafting. In the absence of an aortic or contralateral common iliac artery aneurysm, it would be hard to justify placing a bifurcated aortic stent graft to then accessorize with snorkels. He was not a candidate for the branched iliac stent graft trial (disclosure: I am a site PI for the Gore iliac branched trial and the Cook iliac branched device is also available on trial) and he was not enthusiastic about the follow up -neither was I, when we discussed other endovascular options.
When I broached open surgery, there was a pause because he had read about all the endovascular procedures that were possible, but truthfully, he had never had an honest discussion about open repair.
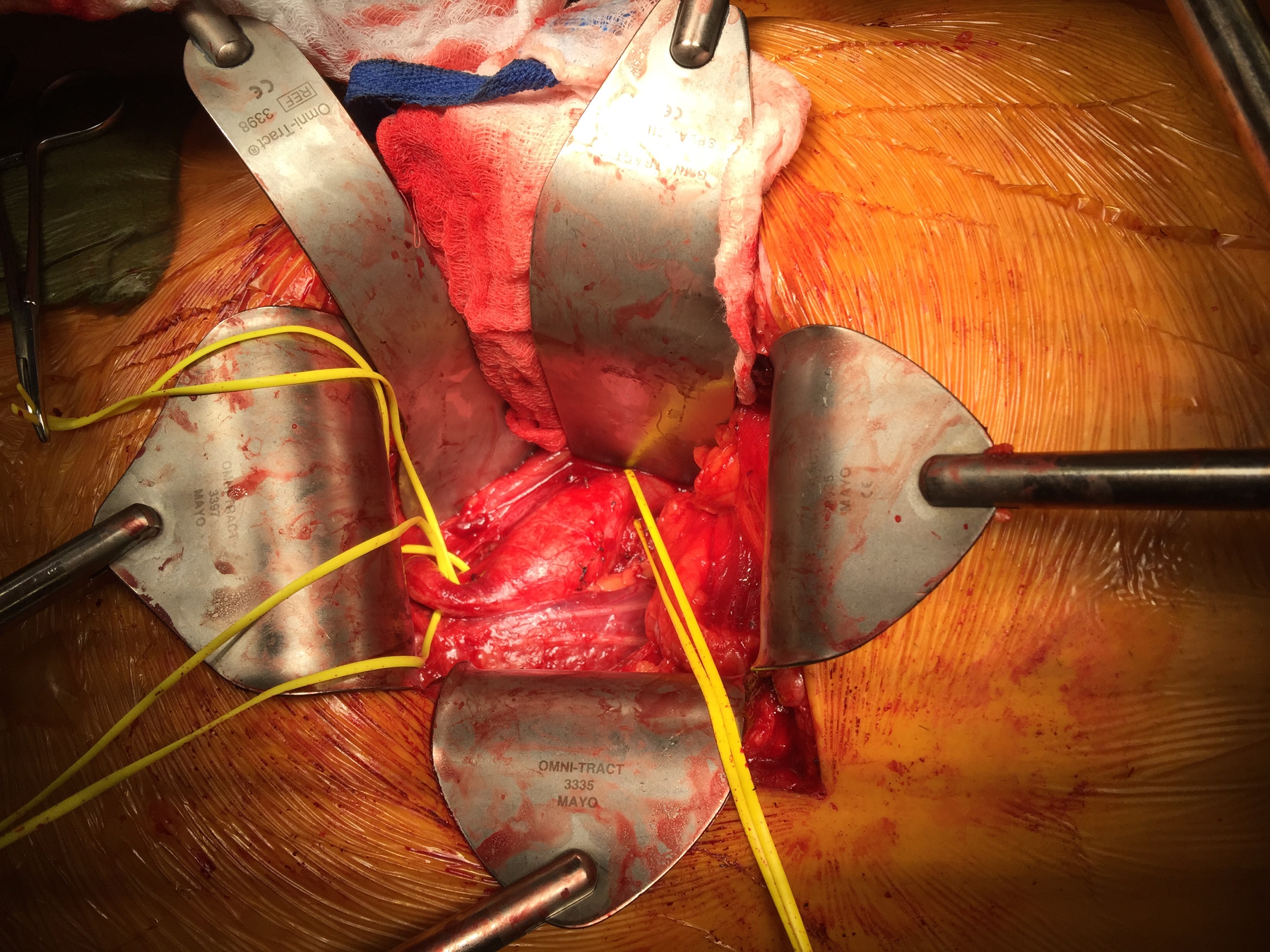
In the current set up of care and training, there would be opinions favoring a purely endovascular approach. Ironically, in another time, the approach we chose would have been considered minimally invasive. The operation was planned with a left lower quadrant retroperitoneal pelvic exposure. The plan was to replace only the aneurysm and revascularize both the internal and external iliac arteries. The internal was revascularized with an end to side anastomosis to a 12mm graft and the common iliac to external iliac revascularization was end to end.

The patient recovered and was discharged in two days. The good thing is that he won’t face buttock claudication and has a low risk of neurologic complications (primarily retrograde ejaculation). Future endovascular options were maintained in the way the graft was tailored -particularly in the creation of a generous landing zone for any future aortic endograft. The patient won’t need to come back for surveillance on the same rigorous schedule as an endograft.

3 replies on “Open repair is preferred for younger patients”
I am the patient in the above post and I can completely affirm what Dr. Park has asserted! My surgery was 6/19/15 and I swam my first mile post-opperatively on 7/3/15 – only 2 weeks later – gradually re-introducing my kick. I am back on my bike riding 15 miles plus at a time and I will be riding a century by next summer! I understand that each patient, their aneurysm and their specifics mandate thorough consideration. However, with the rapidly expanding and improving use of stents, lets not throw out the baby with the bath water and overlook the viability of the “old open repair”! I am eternally grateful to Dr. Park and his team at C.C.
LikeLike
Hey Doc Park! Six years post and life is good! THANK YOU! If ya ever want to fish Lake Michigan again, give me a shout!
Blessings – Pat
LikeLiked by 1 person
Thank you!
LikeLike