In George Orwell’s Animal Farm, under the dictatorship of the alpha pig, Napoleon, the pigs who represented the nomenklatura of the farm chant the slogan “four legs good, two legs better,” after initially declaring “four legs good, two legs bad” during their revolution. They clearly understood the luxury afforded by a bipedal lifestyle, because in rising on two legs, you get arms and hands which can do many things like caress a baby or wield a cudgel. What the pigs in the parable weren’t realizing were the consequences of a bipedal lifestyle.
When Lucy, the Australopithecine, bipedal hominid ran about on two legs, she did have the use of two arms and hands. Possibly an adaptation to living in tall grasslands with few trees, the ability to stand tall like meerkats, allowed the biped to see far into the horizon for big cats who probably loved the big brained hominid for the high calorie meal inside the hard skull -many fossils from this time show puncture marks from the incisors of medium to large cats.
The walking and running put heat stress on the brain, and the tool use which happened incredibly early and is observed in the chimpanzee, likely drove the selection for a larger brain (more neurons will allow for one to lose some neurons to heat stress but stay in the game), but it created likely the first problem for our ancestors -discharging a cantaloupe sized head through a pelvis that was small to begin with but now also reshaped for bipedalism. We still suffer from a childbirth process that no other mammal faces -birthing a less than fully cooked baby -a tradeoff for that giant head.
Standing also meant the load bearing was shifted 90 degrees with long term consequences. For our ancestors who only lived about 20-40 years if the chimps are correct, this wasn’t a big deal as arthritis and tendinitis didn’t preclude eating and breeding and didn’t affect them until they were old. But with modern sanitation and social structures, we are reaching 100 years and the majority of the problems of the integument -the bones and ligament, the low back pain, the sore knees, the ratchety hips, can all be explained by our bipedal lifestyle. Your arm is 30-50 pounds of meat and bone and supported only by muscles off your spine, and your blood vessels and nerves traverse a narrow passage through these muscles and your first rib. Your diaphragm with 5-10 pounds of heart, lungs, and blood sits on first branch artery off of your aorta. Your veins, designed to drain blood from your organs, have to do so with over a meter of static water pressure and your sump pumps only work when you are walking. Muscles and their tendons are stretched tight in the odd way that upright walking and running demands, compressing blood vessels and nerves. All of this weight is put on your feet which have to deal with up to a ton of pressure with running…
I’ve talked about this concept many times before but never had a chance to put it together like this talk. I may write an article. Looking back, I did this blog post (Link).
I am grateful to Ms. Mei Nortley and Mr. John Raphael for the invitation to give this talk.
Median arcuate ligament syndrom (MALS), also known as celiac axis compression syndrome (CACS) and its eponym Dunbar Syndrome, is manifest as epigastric abdominal pain and a compendium of symptoms, arising from chronic compression and inflammation resulting from compression of the celiac plexus between the median arcuate ligament and the celiac axis.
Graphic showing the pathoanatomy of neurogenic MALS (from ref 1). The repeated trauma to the celiac plexus results in inflammation and nerve injury with transmission of pain and neuropathic sensations.
The diaphragm muscle descends from the neck during development (the phrenic nerve originates from C3-C5 nerve roots), and in perhaps up to 25 percent of individuals, drapes across the origin of the celiac axis, and sometimes anchors further down impinging on the SMA or renal artery origins.
While a significant number of patients have this coverage of the celiac axis origin, not everyone has pain. Some whose celiac axis is compressed develop post-stenotic dilatation. For some of these, there is damage to the celiac axis resulting in intimal injury, dissections, thromboses, webs. Turbulent flow causing post-stenotic dilatation in the celiac axis can proceed to aneurysm formation. Downstream in the splenic and hepatic artery and its branches, turbulent flow can engender tortuosity (lengthening) and aneurysms (widening). This disease subset of celiac axis compression should be termed aMALS (arterial median arcuate ligament syndrome).
A question was asked at this year’s VEITH Symposium as to whether post-stenotic dilatation due to median arcuate ligament compression could be considered an aneurysm. The answer given was no, but I think it would be yes in the above example.
Both arterial and neurogenic manifestations of celiac axis compression are under the same ICD code of I77.4, referring to both celiac axis compression syndrome and median arcuate ligament syndrome. While I would never suggest more ICD codes, there should be a differentiation similar to the other compression syndrome, thoracic outlet syndrome (TOS). The pain-based syndrome, which is more common, should be termed neurogenic MALS, or nMALS, and the arterial disease secondary to celiac axis compression should be termed arterial MALS or aMALS. The treatment of nMALS is surgical ablation of the celiac plexus along with median arcuate ligament release, done via open, laparoscopic, and robotic techniques. The treatment of aMALS is the treatment of the arterial complications of celiac axis compression and should involve median arcuate release and treatment of the arterial pathology with either open or endovascular techniques.
Case Presentation
The patient is a middle-aged man with several months of right sided abdominal pain, mostly in the right midaxillary line at the costal margin, right upper quadrant abdominal pain, and right sub-scapular pain. He did not have gallstones, and had no gastrointestinal complaints. He is hypertensive and was on a single agent which he took in the mornings. His pain began during the day and crescendoed in the evening. His prior visits to the emergency room had revealed a hepatic artery aneurysm and celiac axis aneurysm. In the ED, his examination was significant for pain and mild tenderness in the right upper quadrant of his abdomen. He underwent a CT scan.
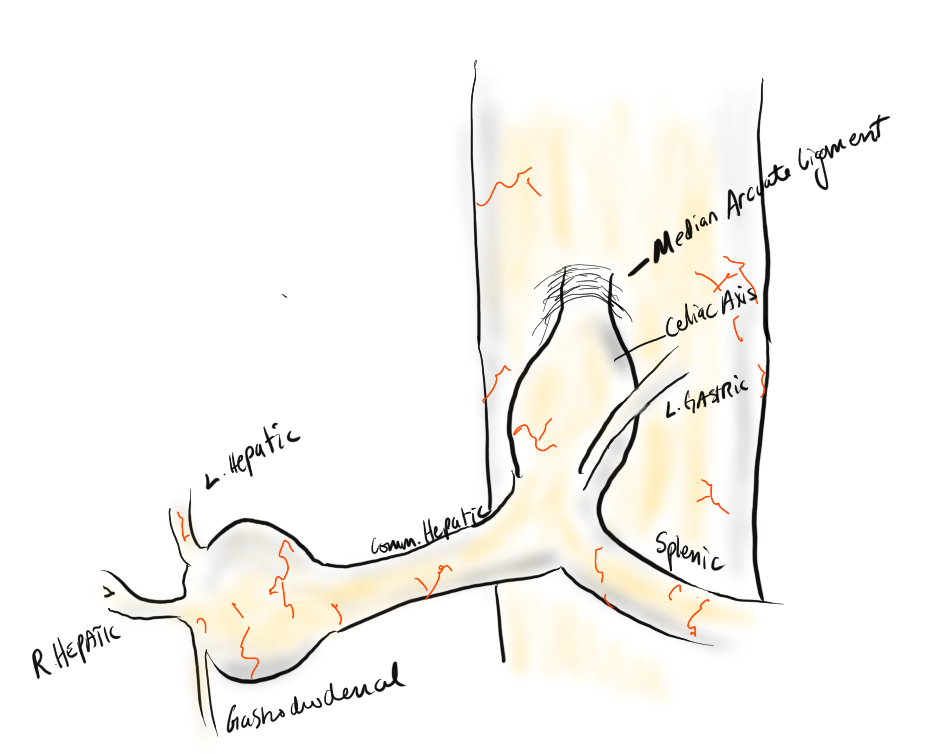
Common Hepatic Artery Aneurysm, 2.4cm with celiac axis ectasia to 14mm, median arcuate ligament compression of celiac axis
The CTA showed compression of the first centimeter of the celiac axis by the median arcuate ligament of the diaphragm and mild post-stenotic dilatation to 14mm. At the terminus of the common hepatic artery, where the hepatic bifurcated was a 2.4cm aneurysm with mural thrombus. With blood pressure control, his pain remitted.
The trainees and I had a lively discussion as to indications for repair and whether this constituted a symptomatic aneurysm. As I have stated in past posts, all pain has a nerve and a mechanism for pain. Abdominal pain and its points of referral are well known going back to the 19th century and encapsulated in Cope’s Early Diagnosis of the Acute Abdomen, whose most recent steward, Dr. William Silen just passed this September. Processes involving the gallbladder and nearby hepatic artery refer to the right upper quadrant abdomen, right chest, right shoulder and scapula which was where the patient’s pain was. And it improved with controlling his hypertension. There was no question to me the aneurysm was symptomatic, likely from strain on the aneurysm.
The question then devolves to whether this is to be done endovascularly or open. While it seems straightforward for me, I have realized at large meetings there will always be some endovascularist proposing something. For me, to exclude pressure from the aneurysm and avoid rupture, the aneurysm had to be isolated from the blood flow and pressure. Ideally, this would be done with tiny covered stents. There are no 7mm x 4mm stents bifurcation stents.
Hypothetical bifurcated small stent system -does not exist, would not work.
Embolization of the hepatic aneurysm, which is done for the splenic, offers hazard of hepatic ischemia. Despite what is written in the textbooks about the portal venous system providing most of the perfusion of the liver, you have to remember there is only portal flow when there is food. Acutely losing one of the hepatics, even clamping it for a time, reverberates as a spike in the LFTs, along with attendant systemic inflammatory response. While the liver, like spleen, can recover and regrow, you mess with it at your great peril. Based on the CTA, closing the hepatic artery with coils and plugs will likely be tolerated as hepatic flow would continue via the gastroduodenal artery which is not small, but there is no guarantee that the aneurysm wouldn’t be pressurized yet by the prominent GDA (if you disagree please feel free to comment).
He was prepared for surgery with echocardiography (normal) and lab testing (normal LFT’s, CBC, BMP, INR), and taken to the OR. A chevron incision was made to broadly expose the area. The median arcuate ligament was exposed and released -there was dense tissues proximal to the dilated celiac axis. The aneurysm was dissected out and the small branches were carefully dissected out and controlled. It is easy to injure the branch hepatic arteries which can constrict on dissection.
A suitable length of saphenous vein was harvested and prepared. The three vessels diagrammed above did not present themselves suitable for a single Carrel patch so I sewed end to end to a patch incorporating the right hepatic and gastroduodenal arteries, and performed a sequential side to end anastomosis to the left gastric artery.
The patient recovered well and was discharged home on POD#5, and in followup had no further symptoms.
Discussion:
The differentiation of arterial and neurogenic manifestations of MALS is an important refinement of our understanding of this disease, which I believe to be a byproduct of our bipedal lifestyle. The lordotic curvature of the spine, necessary to balance our upper torso on a vertical spine, pushes the spine forward and applies tension to the median arcuate ligament, along with other structures such as the duodenum and left renal vein in superior mesenteric artery syndrome and nutcracker syndrome, and the left iliac vein in May-Thurner Syndrome.
This compression is not only enough to narrow the celiac, but injure the artery by crushing. Stenting here does not do well because of the external compression and even after release, the artery may be damaged and require repair.
The chevron exposure heals well and is well tolerated and offers perfect exposure. While I was doing it, it occurred to me that a laparoscopic bypass is technically possible, and may be preferred to the long incision. Recent multi-institution study of MALS treatment would suggest laparoscopic approach offers a lower complication rate compared to open surgery (ref 2.)
The critical thing is having more surgeons recognize the compression that occurs in the abdomen and manifests in disparate and unconventional ways. The key is tying pain to a lesion, a mechanism, a nerve, just the way Cope’s does.
References
Weber JM, Boules M, Fong K, Abraham B, Bena J, El-Hayek K, Kroh M, Park WM. Median Arcuate Ligament Syndrome Is Not a Vascular Disease. Ann Vasc Surg. 2016 Jan;30:22-7. doi: 10.1016/j.avsg.2015.07.013. Epub 2015 Sep 10. PMID: 26365109.
DeCarlo C, Woo K, van Petersen AS, Geelkerken R, Chen AJ, Yeh SL, Kim GY, Henke PK, Tracci MC, Schneck MB, Grotemeyer D, Meyer B, DeMartino RR, Wilkins PB, Iranmanesh S, Rastogi V, Aulivola B, Korepta LM, Shutze WP, Jett KG, Sorber R, Abularrage CJ, Long GW, Bove PG, Davies MG, Miserlis D, Shih M, Yi J, Gupta R, Loa J, Robinson DA, Gombert A, Doukas P, de Caridi G, Benedetto F, Wittgen CM, Smeds MR, Sumpio BE, Harris S, Szeberin Z, Pomozi E, Stilo F, Montelione N, Mouawad NJ, Lawrence P, Dua A. Factors Associated With Successful Median Arcuate Ligament Release in an International, Multi-Institutional Cohort. J Vasc Surg. 2022 Oct 25:S0741-5214(22)02443-0. doi: 10.1016/j.jvs.2022.10.022. Epub ahead of print. PMID: 36306935.