

I had posted the above picture from over 15 years ago during my time in Iowa of my hybrid AUI-Fem-Fem (under unclampable 2, link). This technique came back to me as I was strategizing the upcoming aortic revascularization of a patient with iliac occlusions with the added complexity of an ileal conduit in the right abdomen. He had multiple failed prior iliac stents and failed femorofemoral bypasses -his right CIA and EIA were occluded while the left EIA had become occluded resulting in ischemic rest pain. While the picture alone is sufficient for me, it was brought to my attention by Dr. Joedd Biggs, fellow alum of the Mayo Clinic, on faculty at University of Kansas Hospital, that more detail was needed. So while resting my tired dogs, I got on my tablet and drew it out. Joedd, I present you my technique for a hybrid AUI-Fem-Fem bypass of the aorta.
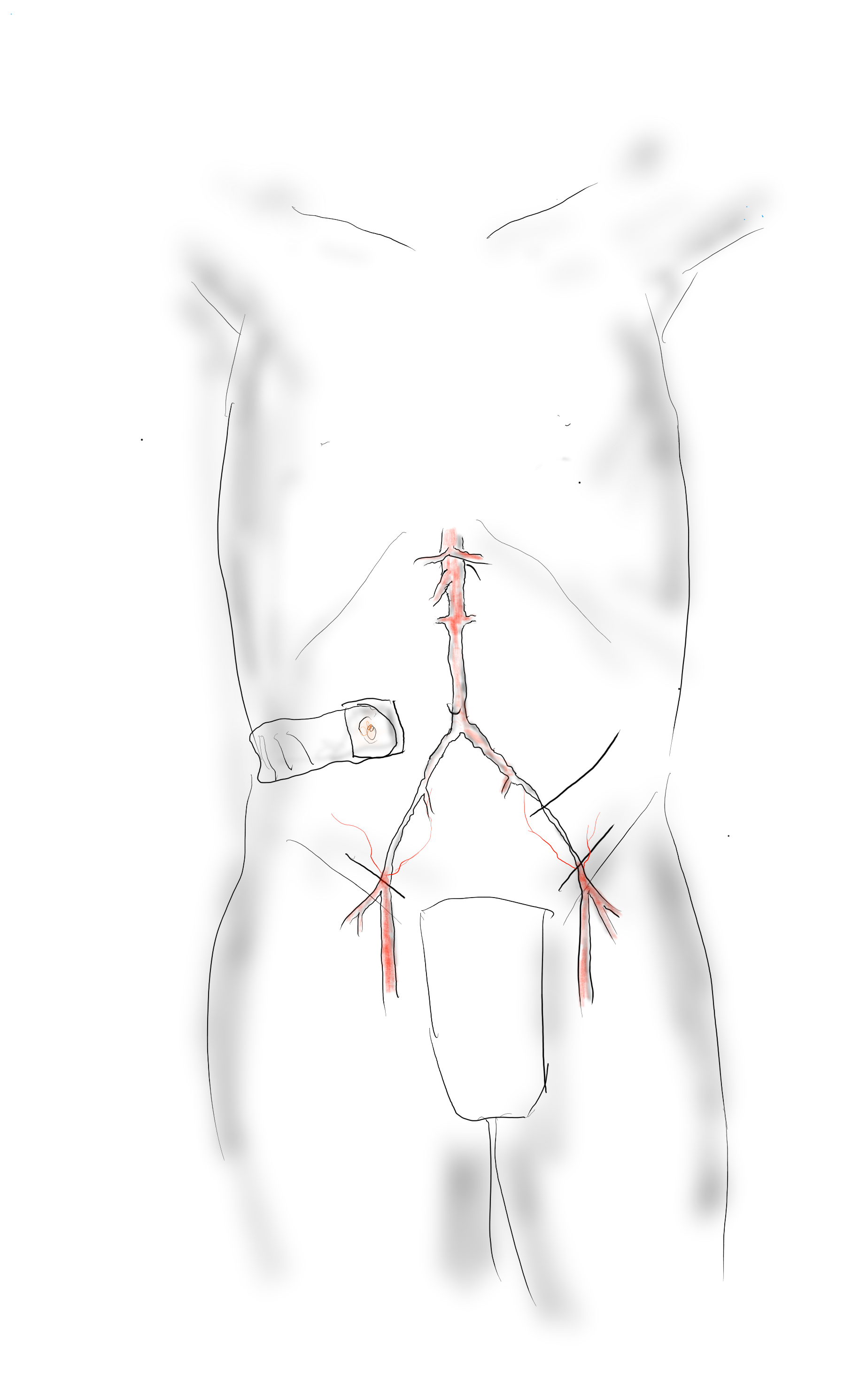
The image above shows the necessary incisions for the femorofemoral bypass and the retroperitoneal pelvic (transplant) exposure of the left iliac bifurcation. I nearly always make oblique rather than vertical skin incisions in the groin to avoid wound complications from incising the inguinal crease orthagonally.

A left lower quadrant retroperitoneal exposure of the pelvis is performed -this is a standard renal “transplant exposure.” The two groin incisions are made and the common femoral arteries are exposed. Endarterectomy may be performed, although if the orifices of the SFA and PFA are patent, I don’t. The bypass graft is tunneled retropublicly and this is facilitated by the transplant incision. I generally use a 7mm ringed PTFE graft. Once done, the common iliac artery is divided above its bifurcation and the bifurcation is oversewn or stapled. A 12mm bypass graft is then sewn end to end to the common iliac artery (below).

Through the conduit, a suitably chosen iliac limb of an EVAR system is brought through to the aorta and deployed with its end across the anastomosis into the conduit. A Gore Excluder 12mm ending iliac limb is ideal as its proximal end is appropriately sized for the diseased abdominal aorta. The limb is then aggressively ballooned to profile, particularly in the 12mm graft (below).

The 12mm conduit graft is then sewn end to side to the femorofemoral bypass (below), completing the AUI-Fem-Fem.

I believe there are hemodynamic advantages to this over reintervening on native aortoiliac segment. First, size does matter, and until a suitable aortoiliac occlusive disease stent graft system is engineered, this represents an optimum. The Gore excluder graft limb is 16mm proximally and this is usually more than enough to diameter for the diseased abdominal aorta. The end diameter of 12 or 14.5mm will seal nicely in a 12mm conduit. I have not used a 16mm conduit only because I prefer not rupturing the aortic bifurcation with the “aggressive ballooning” mentioned above. The 12mm diameter is the boundary above the “small aorta syndrome” diameter of 10mm.
If the iliac is occluded, a wire can be driven through it from above and the conduit sewn over it. The iliac limb can be delivered after some pre-dilatation then followed by the “aggressive ballooning” of the iliac limb. The deployment into the conduit creates a stable “endo-anastomosis.”
Patients like my upcoming patient usually fail intervention due to the lumen size issues. An 8mm fem-fem bypass fed by a diseased series of iliac stents with at most 7mm lumen diameter is a recipe for the development of mural thrombosis and occlusion. The lower half of the body are fed by the diseased conduit of the donor EIA. This way, true aortic inflow is created.

2 replies on “hybrid AUI-Fem-Fem technique”
Thanks for sharing this! Best,
Jose
LikeLike
Marvelous case
LikeLike