
5 Top FAFO’s In Vascular Surgery
In no particular order, I list these problematic situations that are outsized in their ability to take a case sideways.
- Ischemia syndromes in the unconscious. The unconscious tell you nothing about their pain and follow no commands. Therefore, vigilance and a low threshold for operating are what will save the patient if they are salvageable. Objective evidence of flow -examination, handheld pulse Doppler, duplex ultrasound, CT angiogram, exploration and visual inspection, must be obtained. The typical scenarios are dissections of the ascending thoracic aorta, polytrauma patients, and patients on ECMO. By the time the dissection is repaired and the patient is off pump, they may be long past the 6 hour threshold for irreversible ischemia for gut or muscles. The patient involved in a rollover MVA who had their femur fracture reduced after ten hours waiting on the add on schedule should have their compartments assessed visually through fasciotomies. Patients on ECMO via femoral access must by practice have distal perfusion cannulation. Assessment for ischemia need to start at admission for the unconscious patient with assessments of flow and function. Waiting until markers of cell death are apparent on blood tests is not the right approach unless the patient is DNR.
- Operations in redo or irradiated fields. Preparation and coordination is key. Most vascular surgeons have a plan for controlling arteries and veins in these settings, but a common scenario is in trauma or oncologic surgery. I don’t know if anyone has done this, but the idea comes to me that if there is concern for oncologic invasion of a major artery -an aorta or iliac, it would be reasonable to place a wire, balloon, or stent graft across that area with solid seal zones to allow for free dissection and resection of any involved artery.
- Central venous rupture during venoplasty for hemodialysis access with an open fistula. Instead of venous pressures, with a fistula attached, arterial pressure is driving the leak. A leak of an SVC can lead to a fatal cardiac tamponade. Because the heart fails to fill, CPR is futile. The only thing can be done once this has occurred is to be prepared to a. ligate the fistula, b. Drain the pericardium either with needle pericardiocentesis or left anterior thoracotomy. Better still is preparing for SVC venoplasty by balloon occluding the fistula prior to inflating the balloon in the SVC.
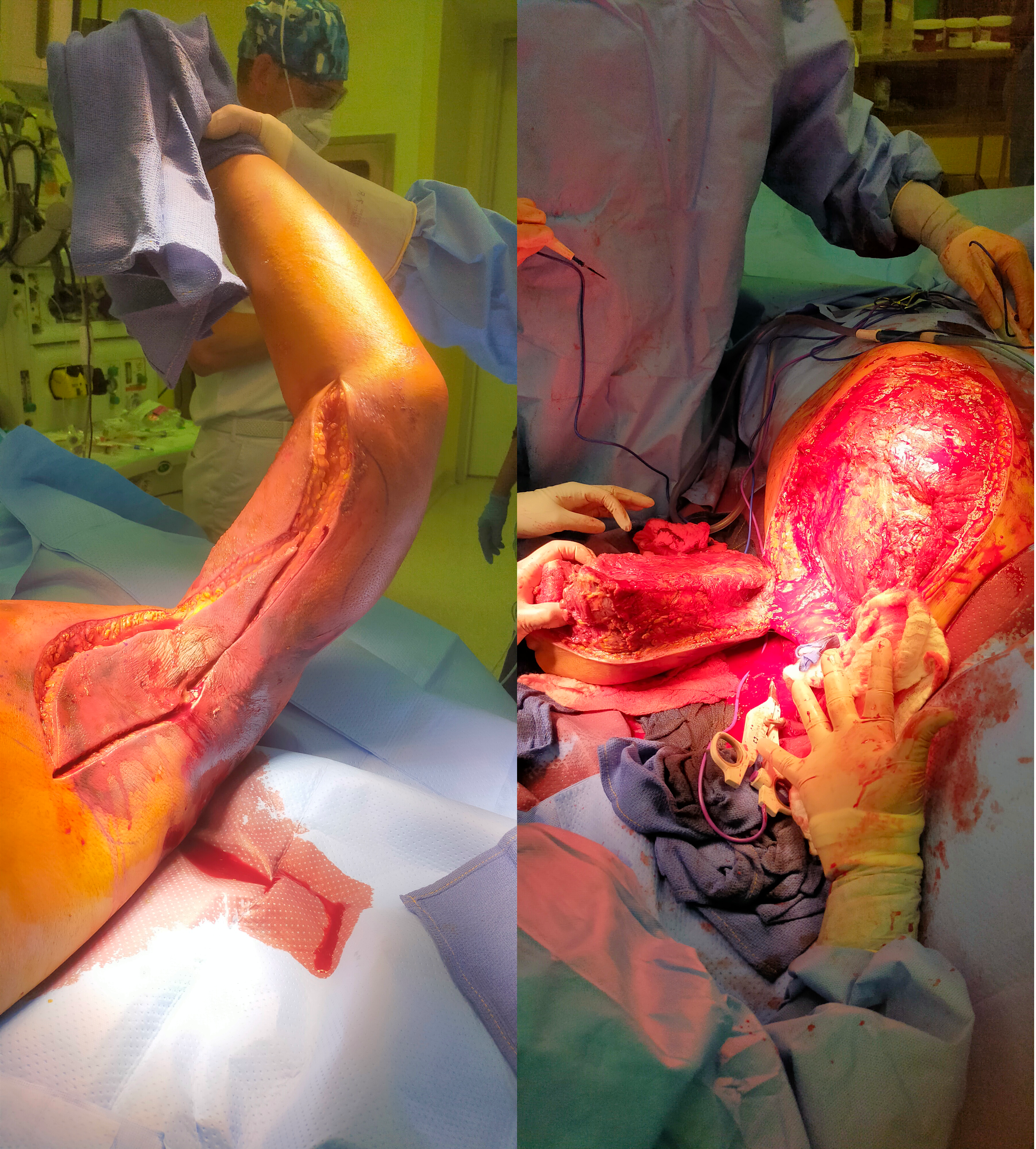
- Rapidly progressing skin infections. It is amazing how fast necrotizing infections can progress. I’ve seen simple infections of a finger spread to the whole arm over the course of an hour or two in the waiting room of an emergency room. There are forgotten anecdotes of medical students dying after nicking their hands in gross anatomy. I saw a concert pianist lose her arm after getting a thorn from her rose garden. The image below is of a forequarter amputation I had to perform on a young man with a fulminant infection of the muscles of the left upper extremity undergoing a forequarter amputation after an overnight of misdiagnosis as a cellulitis at an outside facility. It grew among other things Candida auris, a terribly frightening organism and spread to his chest wall and ribs, resulting in death.
5. Iliocaval venous injury, particularly small tributaries going under aorta or around its branches. While not pressurized, they have tremendous flow like a hole in a plastic bag holding a goldfish, and without precise control, you are as likely to widen the hole or make more holes as you try to suture the holes. I’ve had some success using the Park clamp (link). You can’t buy one but you are free to have one made by your local smith. Otherwise, you need to keep your finger on the hole while you call in help, usually in the form of more vascular surgeons to get exposure and the vein properly clamped for repair.

Add yours in the comments below.

5 replies on “Top 5 FAFO’s in Vascular Surgery”
Dr. Park, my name is Sebastian Slazyk and I am a 30 year old male that is having a hard time getting a diagnosis after a dental surgery a year ago destroyed my health. You seem to be very well versed on these topics and don’t know who else to reach out to. Shortly after dental suregry experienced severe stomach pain and general body tiredness and muscle weakness. After 6 months of investigating MALS and other vascular occlusions have been found. Currently scheduled to MALS release in Dec but I fear vasculitis as perhaps an underlying cause to my issues. Please any help or advise would be amazing.
LikeLike
Vasculitis can be investigated through blood testing with a rheumatologist
LikeLike
I did have the typical blood work done with CANCA and PANCA being negative, along with c reactive and esr being negative. The only clue was a slightly elevated ANA and elevated alpha lambda ratio. More so my CT Angiogram has shown severe stenosis of the celiac artery (100 blockage with retrograde blood flow) and left renal vein stenosis and testicular pain. I know while rare, some cases of vasculitis can present with negative blood work. Any thoughts or suggestions on rheumatologists who would be worth while to talk to?
LikeLike
You have an increasingly common presentation of combined MALS and Nutcracker Syndrome with gonadal vein reflux into testicle. You get pain with eating and when you stand for long periods you feel like you are kicked in the balls? Need to see a vascular surgeon.
LikeLike
I would add proximal control for junctional vascular trauma. I’ve had a few proximal carotid/subclavian penetrating traumas where the expeditious neck exploration and median sternotomy required a well coordinated team to prevent rapid exsanguination.
LikeLike