
Tinkering in the basement, because bringing a laparoscopic tower and simulation setup into my house would be difficult.
Category: techniques
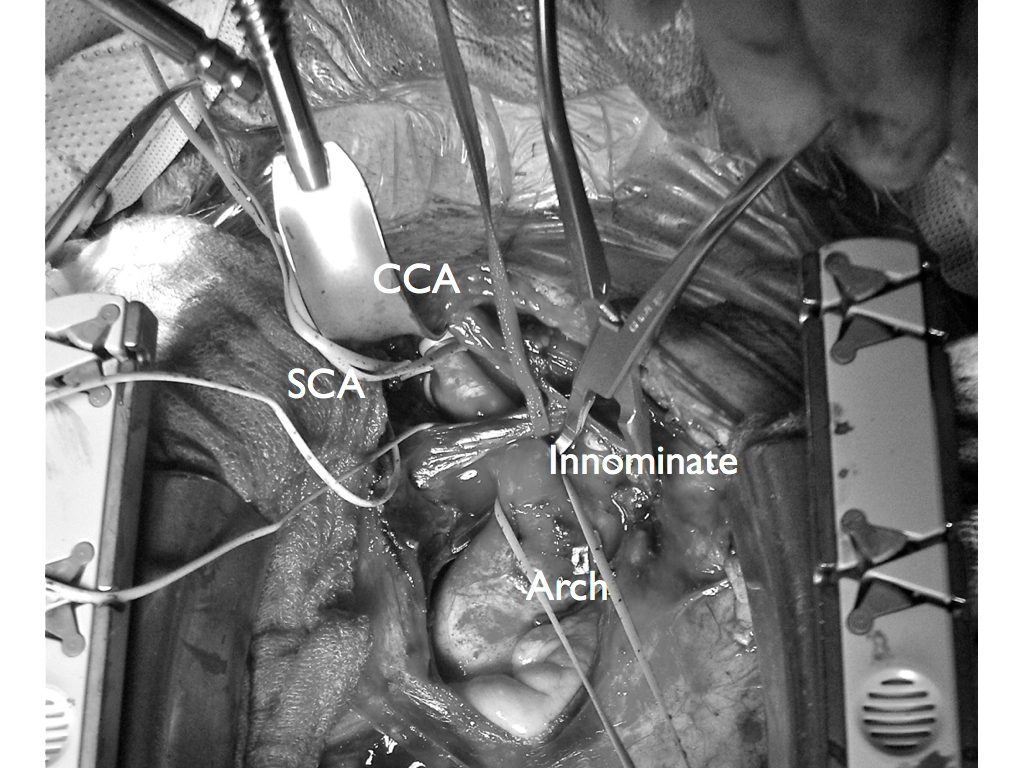
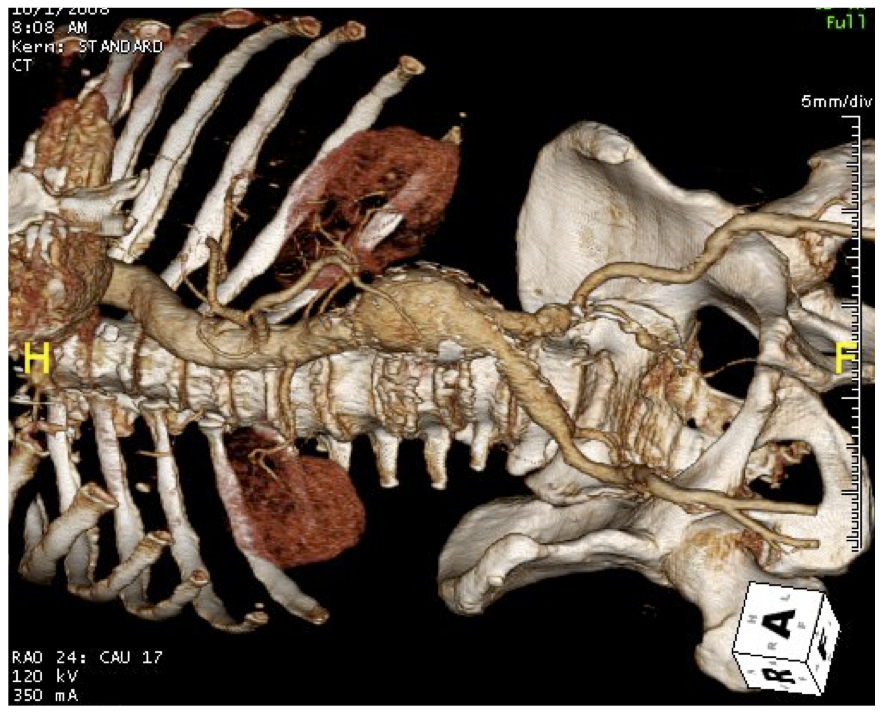
The patient, a 47 year old woman, was referred for syncope, but it was much worse than that. Excessive stress, standing, and thinking hard were described as causes of her syncope. Frequent headaches and lethargy lead to inability to keep a job. Several MVA’s resulted in revocation of her driver’s license. Added to that was a two to three pack a day cigarette habit. Her cardiac workup was negative, but it was noted that her carotid duplex was notable for a left ICA occlusion and left vertebral occlusion. Blood pressure in both arms was in the 70’s systolic while in her better thigh it was 90’s. She had an open right carotid system but the flows in the common carotid were attenuated. CTA of the arch revealed severe arch disease affecting the origins of her great vessels. The innominate artery was severely diseased to its bifurcation with a small <2mm channel of flow. She had a dominant right vertebral artery that was patent, and the right ICA had moderate disease at its origin. This was in 2009, and I entertained intervention, but wasn’t all that confident that kissing stents into the innominate was all that great of an option even though there are reports of innominate interventions in the literature. I had the opportunity to perform a handful of great vessel reconstruction with Ken Cherry during my fellowship and felt that this was an ideal case for an innominate endarterectomy.
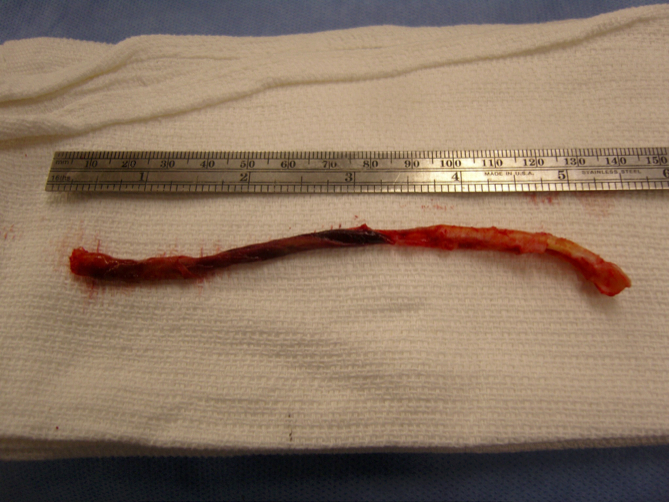
This is one of those rare and infrequent cases from vascular surgery history. The exposures is one of the grand vistas of vascular surgery. The arch, thankfully, was only calcified at the origins of the vessel and clamped well. The endarterectomy was not that much different from an aortoiliac endarterectomy with a fibrocalcific plaque and was extended onto the common carotid while the origin plaque of the subclavian was plucked cleanly. The phrenic and vagus nerves were protected. The patient was centrally hypertensive as found by a long femoral arterial line and was kept that way for the duration of the clamp. A bovine pericardial patch was applied and the sternum was closed over a mediastinal chest tube.
The recovery was impressive for the patient’s immediately improved state of consciousness, lack of lethargy, and improved cognition. She was herself impressed enough to quit smoking during that admission for good. Her right brachial cuff pressure now correlated well. She went home POD 5. When I last saw her 2 years later, she was employed and symptom free with continued patency of her repair, consistent with the earlier reports of this operation (Cherry et al. J Vasc Surg; 989;9:718-14).

From my archives, the CTA illustrates two points. First, tunneling can be done without taking down much of the retroperitoneum. This lesson came to me after taking a course in laparoscopic aortic surgery with Dr. Dion in Quebec City. The old BARD-IMPRA tunnelers with their bullet tips -the short gently curved one, is particularly well suited for tunneling from the groin to the aorta -if you have a hand on the retroperitoneal pelvis, it is very straightforward to guide the tunneler to the proper location. The other point is that the graft is applied proximally end to side with a leftward orientation. This combined with dissection of the retroperitoneum with a large Ligasure or harmonic scalpel lets you avoid the problem of having no tissues to close over the graft. You take down the retroperitoneum with a cuff of tissue of about 5cm from the duodeum. Normally, this can be bloody but with the energy devices, it is not. This provides excellent graft coverage. You just have to mind the IMV which may or may not have to be taken down. End to side is preferred because you preserve endovascular options, but in this case, the anastomosis was done end to end.
April 30, 2009 11:33 PM
Aortic Bypass for occlusive disease
The patient arrived with the history of severe claudication. He was a middle
age smoker whose job required walking several miles a day. This became
increasingly difficult until he was clearly limping at short distances. He was
also developing cramps in his legs at night, worse in his left leg.
On examining him, he had no pulses in his left leg from the groin down.
The pulse volume recordings (PVR’s, red lines) on the left clearly
demonstrate normal flows in his right leg with sharp upstrokes, dicrotic
notch, and shallow diastolic relaxation. The left leg had attenuated flows on
the pulse volume recordings with dampened, gradual series of mounds.
The flow was flat at the metatarsal level (foot). His ankle brachial index
( BI) on the right leg was 0.75 which was mildly depressed. The ABI on his
left leg was 0.43 which was severely depressed.

CT was performed (above left) showing that his left iliac system was
occluded. This is due to atherosclerosis which is a systemic disease. This
kind of blockage can occur in any organ, but it was most severe in this
patient’s leg. His right common iliac artery also had moderate plaque.
He underwent an aorto-right iliac and left femoral artery bypass with a
bifurcated graft (above right). This greatly improved flows in his left leg, with
his BI improving to 1.05 from 0.43. The PVR’s also reflect this improved
flow. The right leg, surprisingly, also had an improvement despite not
having a severe stenosis in his common iliac artery. The fact is, the
common iliac artery, but being heavily diseased over the length of the
artery, offered a hemodynamically significant stenosis despite being patent.
His BI on the right improved from 0.75 to 1.03.

The operation was done with minimal invasiveness in mind. The CT
allowed for planning of the abdominal incision directly over the part of the
aorta requiring operation. The groin incision on the left was created
obliquely as to avoid crossing the groin crease -which I believe increases
the chances for tension on the wound and subsequent infection. The graft was tunneled without mobilizing the sigmoid colon directly up to the bifurcation using an IMPRA tunneler -by placing the hand in the pelvis, the
tunneler can be felt and guided in the correct trajectory. The graft was a
Gelsoft Plus graft soaked in Rifampin. This antibiotic bonds to the gelatin in
the graft giving protection against indolent bacterial infections for about 3-6
months after the procedure -this is helpful especially with groin incisions. The operation took 2.5 hours and the patient went home within a few days.
The patient is now walking without pain and will be returning to work. He
has also successfully quit smoking which has a significant impact on his
risks of future heart attack, stroke, or peripheral vascular complication. His
relative youth (in his fifties) required that we give him a repair that would
give him the best chance at maintaining patency for many years. The aortic
bypass graft for occlusive disease has a proven track record with patency
measured in decades.
From my notes
November 7, 2008 9:05 PM
Using TeraRecon for planning minimally invasive aortic surgery
Terarecon, Vitrea, Osirix, all allow for visualization of three dimensional CT data. The 3DVR (virtual reality) view, is often overlooked, but is an important feature of Terarecon. It is a synthesis of the axial data and does for you what you tried to do in your head back in the days of cut axial film -that is reconstruct a three dimensional picture from 2 dimensional sections. This is a moderate risk patient, 65 years of age, with a 5.8cm AAA. The top image shows the standard 3DVR perspective with the surgeon standing on the patient’s left. By adjusting the levels, you can bring in the organs (not shown), and then the muscles (panel below).

You can then bring in the skin by manipulating the “window levels” -in TeraRecon this is done by pressing both left and right mouse buttons. This allowed me to plan the location of a skin incision (measuring 15cm) for a minimally invasive AAA repair.

While 15cm hardly qualifies as a mini-laparotomy, it is less than half the length of a “stem to stern” laparotomy.

Dr. Jon Cohen et al. reviewed their experience with laparoscopic versus minilaparotomy averaging 8-10cm in length, and found that OR time, fluid given, and length of stay was superior in mini-laparotomy compared to open and laparoscopic assisted repair (ref).

I would say that learning curve probably accounted for the difficulties with laparoscopic-assisted. In this patient the tube graft AAA took 2.5hrs, and patient was extubated post op and went home in 4 days. TeraRecon made short work of planning out the location of incision and was predictive of the viewing perspectives.
Addendum 11/30/2014
Using the 3DVR perspectives in thoracoabdominal aortic aneurysms is indispensable for planning retroperitoneal thoracoabdominal exposures, and I will post an example.
reference
J Vasc Surg 1999;30:977-84

From my case files, this was a case which I performed in 2010 and published in a prior blog.
CCx: Patient is a 56 year old man with complaints of pain in right leg with walking short distances and discomfort in the foot at night.
HPI: The patient has had cramps in his right calf with walking about a block for over a year, but over the past three months, he has developed pain with walking less than half a block which is incapacitating. He has developed pain at night which wakes him and he has taken to sleeping with his right foot dangling off the edge of the bed. This has resulted in some swelling of that leg which makes it doubly uncomfortable to wear shoes. He works as a manager at a local big box store and walks constantly. He used to smoke but quit last week. He feels this has worsened the pain.
Past Medical History: Hypertension, dyslipidemia, acid reflux
Past Surgical History: Ruptured appendix at 22
Medications: Zantac, Hydrochlorothiazide, Lipitor, Aspirin
Allergies: Penicillin (rash in 1972)
Social History: Employed, 30 pack year smoking history, quit last week
Examination: T 98 BP 142/88 HR 88 RR 12 Ht 68inch Weight 192lbs
HEENT: PERL, EOMI
Chest: Bilaterally CTA
Cor: RR
ABd: Soft, scar right lower quadrant
Ext: Cool right foot with dependent rubor, elevation pallor. Warm left foot
Neuro: Motor and sensory examination normal
Skin: Loss of hair over toes of right foot, and distal right leg pretibium
Pulses: No palpable pulses right leg. Left leg femoral, popliteal, and dorsalis pedis artery pulses are easily palpable
Labs: WBC 9.8 Hb 13.2 HCT: 40 PLT 332 Cr 0.8
Testing: Segmental pressures R/L: Brachial 144/138 High Thigh 88/150 Low Thigh 77/140 Calf 72/132 Ankle 71/140 Metatarsal 68/122
Pulse volume recordings notable for moderately diminished signals right high thigh cuff.
CTA: Moderate atherosclerosis of infrarenal abdominal aorta and its bifurcation with severe plaque of the right common iliac artery and occlusion of the external iliac artery. There was reconstitution of the common femoral artery on the right via collaterals. The left common iliac artery was affected by a moderate (50-75%) stenosis due to low density plaque.
Impression: PVD with rest pain of right leg due to severe aortoiliac occlusive disease and occlusion of right external iliac artery.
Plan: After discussing treatment options, we decided to try a right external iliac artery remote endarterectomy with angioplasty and stenting of his common iliac disease. This was chosen over aorto-bifemoral bypass because he had limited time off from work and work did require that he lift more than 20 pounds.

Operation:
Remote endarterectomy of right external iliac artery with aortography, bilateral common iliac artery angioplasty and stenting.
This operation was done via a single right groin exposure and percutaneous access of the left groin. The common femoral artery had severe posterior plaque which was the starting point of the endarterectomy. Up and over access of the right external iliac artery was achieved and a wire was passed across the occluded external iliac artery and into the right femoral system. With clamping of the common femoral artery, the wire was brought out and controlled with a Fogarty clamp -this allowed for excellent stabilization and control and possible emergent balloon occlusion in the case of a perforation.
A Vollmer ring dissector was sent over wire and plaque up the external iliac artery under fluoroscopy and dissection was stopped at the iliac bifurcation which was heavily plaqued. A Moll Ring cutting device (LeMaitre) was used to transect the plaque which was removed.
The right and left common iliac arteries were stented with self expanding nitinol covered stents and post-dilated. I chose this as I have had occlusions occur in the setting of diffuse TASC C disease with low density plaque -I suspect that thrombus propogates across open cells like weeds growing through chicken wire. The stents on the right were extended across the iliac bifurcation.
A completion angiogram is here to the right. The common femoral artery was repaired with a patch angioplasty (bovine pericardial patch, LeMaitre).
The groin was closed and the patient recovered and was discharged in a few days with excellent palpable pulses on the right and improved pulses on the left. He was without symptoms of claudication or rest pain in the right leg.
Discussion:
Remote endarterectomy allows for removal of plaque via a single groin incision, obviating the need for an abdominal exposure required in an aorto-bifemoral bypass. This minimally invasive technique is associated with a low complication rate and earlier return to full work status because the abdominal incision is avoided.
Smeets et al [reference] reviewed with 7 year experience with 48 patients and had a technical success rate of 88%. One patient died due to a myocardial infarction within 30 days of the operation. The complication rate was low. 6 patients required coversion (retroperitoneal flank exposure) for additional arteriotomy (3 patients) and bypass (3 patients). The primary and assisted patencies shown to the right were acceptable with a secondary patency of 94% at 3 years.

These cases require more surveillance than an aortobifemoral bypass. Intimal hyperplasia does occur in random loci in the SFA remote endarterectomy and this should apply to the external iliac artery. I chose the title because the external iliac artery biologically behaves like the superficial femoral artery in relation to endovascular patencies and not like the common iliac artery or aorta -probably because it shares a common embryology with the SFA, not the CIA. It is a troublesome artery that is often overlooked by vascular surgeons when femorofemoral bypass is performed for occlusive disease -the supplying external iliac artery though patent is usually diseased and has a small lumen. With a fem-fem bypass, both legs are supplied often through an artery with the caliber of a child’s drink straw. I have seen the donor leg become symptomatic through what is termed steal, but in fact reflects the hemodynamic inadequacies of a diseased external iliac artery.
I feel that 5mm is the minimal lumen caliber for an external iliac artery, and a 4mm lumen in an adult will clearly show a hemodynamic effect particularly after exercise or application of vasodilators in the endo suite. Stenting an occluded external iliac artery though technically feasible even in this case is not a durable solution in my experience. This operation allowed the patient to return to work without an extended convalescence.
I think removing the plaque offers advantages over stenting to the inguinal ligament. The common iliac stents have superior potency to external iliac artery stents and moving the stent point to the CIA and not stenting the EIA in my experience has better long term potency.
Reference
Smeets L, et al. J Vasc Surg 2003;38:1297-1304.

The patient is a baby who had undergone cardiac catheterization prior to repair of tetralogy of Fallot. Postoperatively he developed acute limb ischemia and was found to have an occlusion of his left common femoral artery. This was unusual, as typically, these babies tolerate catheterization and a high rate of CFA occlusion without ill effect. Usually treatment with heparin for a period of time is sufficient. In this child, there was clearly severe ischemia. What was different about this child was that his mother and her two siblings suffered from severe Raynaud’s disease, suggesting in this baby, vasospasm played a role. The foot was cold and not moving, and there were no signals from the groin down. The baby was taken to the OR for a CFA exploration and thrombectomy, as I felt the likelihood of infarction in this baby was high. The common femoral artery was exposed via an oblique incision and it was about 2mm in diameter, translucent, and very elastic. There was thrombus and I performed a longitudinal arteriotomy. There was minimal thrombus and a gossamer dissection flap. Inflow was easily established. There was no backbleeding.

Repairing the artery was initially not straightforward. The available nearby vein was even smaller for lack of blood flow and in spasm, and primarily repairing it was not a good option. There is literature describing patch angioplasty, but I felt there had to be a faster, better solution that did not require 8x magnification. Then it struck me that the artery was so pliable that it was every easy to mobilize a length of it from under the ligament.

My inspiration was the Heineken-Mikulicz pyloroplasty. 
Once the laterally oriented stay sutures were in, interrupted (always) 8-0 sutures created a nice repair.  The blood flow was high resistance, but the outcome was immediate. The baby had had over two days of ischemia, and I did go ahead and perform fasciotomies of the leg. There was dead muscle in all the compartments, but with VAC therapy, the baby healed within a few weeks, and a year later came in walking without a limp!
The blood flow was high resistance, but the outcome was immediate. The baby had had over two days of ischemia, and I did go ahead and perform fasciotomies of the leg. There was dead muscle in all the compartments, but with VAC therapy, the baby healed within a few weeks, and a year later came in walking without a limp!


At last week’s Veith Symposium, there was a straw poll for parallel grafts versus fenestrated stent grafts in emergent setting, and the results were a populist parallelist majority. This is clearly the result of years of inability to access this technology and reflects market forces making the decision over careful science. There are clear examples of this in the past -the adoption of laparoscopic cholecystectomy and appendectomy, done without randomized control trials shows that RCT’s be damned, people and surgeons will get what they want.
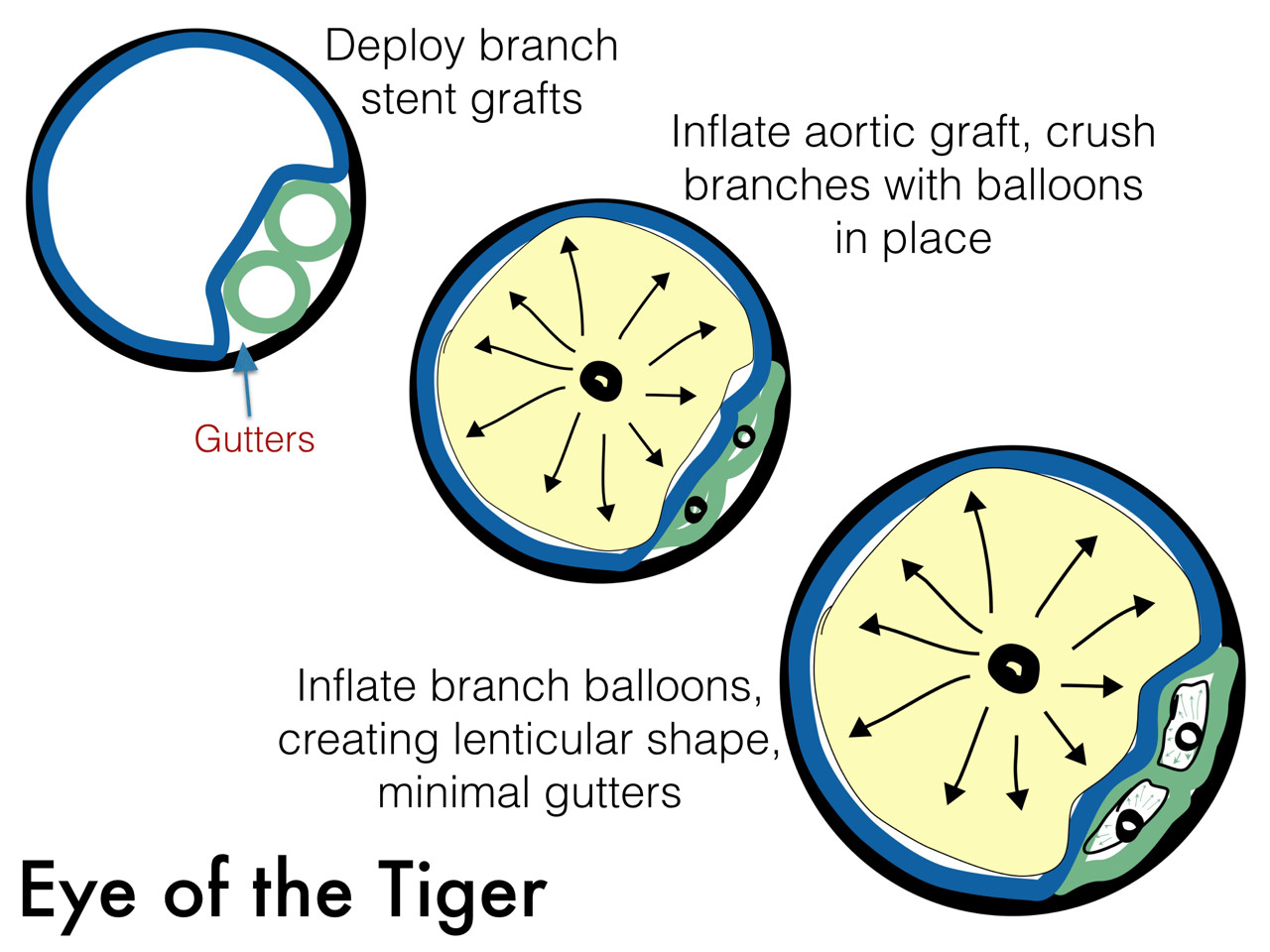
The several presentations on parallel grafts caught my eye. First was the Eye of the Tiger technique which sounds like a kung-fu move. Presented by Dr. David Minion of the University of Kentucky, the gist of it is that the gutters created by parallel grafts can be obviated by reshaping the branch grafts from circles to lenticular shapes (illustration). The sequence of moves is to deploy a balloon expandable stent graft outside of the main graft and deploy it, then deflate the balloon. The aortic graft is then ballooned, crushing the branch graft. With the balloon inflated, the branch graft is then inflated, now taking a lenticular configuration. This, I will put in my tool box.

The other presentation was on the bullfrog catheter, by Dr. Christopher Owen of UCSF. It inflates to press the catheter portion of it in the middle of the length of the balloon against the stent graft wall. A penetrating needle then comes out through the graft material, allowing for infusion of a sealing embolic material. This has not been tried in humans but application in an animal model is ongoing.

I have a feeling parallel grafts will be with us for a while. Using these in conjunction with the Nellix graft, juxtarenal aortic aneurysms were treated, which brings me to think that with the inevitable progression of paravisceral segment aneurysm disease, we will be seeing secondary endobags (not a pejorative) for treatment of paravisceral aortic aneurysms with parallel grafts, and we will see something like this on CT scans one day (illustration). Mr. Ian Loftus of St. George’s Vascular Institute reported on 19 patients (11 single, 5 double, 3 triple branch) over 12 months who were unsuitable for OR/EVAR solutions, treated with 100% technical success, one type I endoleak. Dr. Michel Reijnen presented the Arnhem experience with this technique. Their series included 7 patients with juxta (5) or para (2) renal AAA’s (4 single, 2 double). He reported 100% chimney graft patency and no reinterventions in short followup. He presented a case of rupture, but warned that further investigation would be needed before using the endobag for rAAA.
I think that the whole issue points to several truths. Paravisceral and thoracoabdominal aortic aneurysms have always been viewed with trepidation and this generally caused referral of these cases to high volume centers and surgeons during the open era. Experience with EVAR has infused a sense of confidence and with mastery of infrarenal EVAR and basic endovascular interventions, most practitioners feel ready to offer an endovascular solution to the visceral segment AAA’s, but feel locked out either through lack of training or inability to access the devices, particularly not having ready solutions on the shelf. These parallel graft systems offer relative ease of delivery and use readily available components. Even I have resorted to parallel grafts in an emergency with acceptable short term result (patient lived) but with uncertainty with durability.
I think that there will never be a completely satisfactory off the shelf, “every-surgeon” solution because these patients are no less complex when approached with endovascular technique -they just present a different set of equally difficult challenges. As in open repair of these complex aortic aneurysms, endovascular repair of these should aggregate to high volume practices and centers with deep experience.

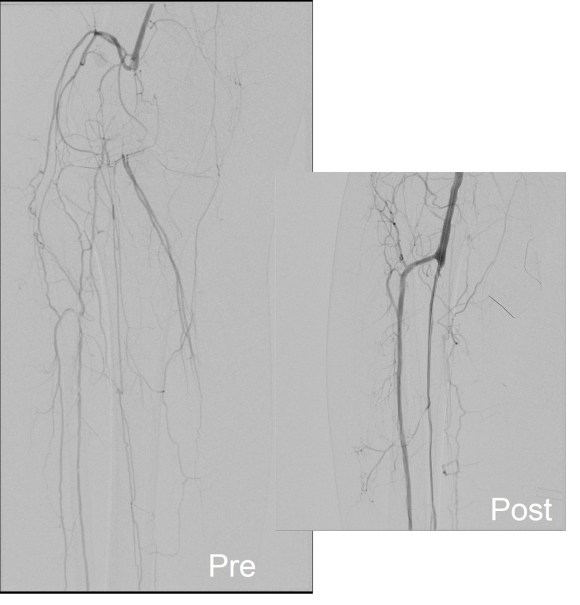
The patient is an elderly woman who had severe rest pain due to popliteal artery and tibial occlusion. She had no leg veins and sparse arm veins which would have to be spliced to achieve a femoro-peroneal bypass. Her preop CTA showed a patent SFA and proximal popliteal artery occluding above the joint and reconstituting only the peroneal artery. I planned for a retrograde popliteal remote endarterectomy tibioperoneal trunk endarterectomy via a below knee exposure with patch angioplasty of the arteriotomy, the bailout would be a short arm vein bypass from the above knee popliteal artery to peroneal artery.
Arteriography was performed via a left common femoral access and is shown below.


The popliteal artery was occluded and there was a very small peroneal artery that continued down the leg with seeming occlusion of the anterior and posterior tibial arteries. The popliteal and anterior tibial artery were exposed through a below knee incision taking care to avoid venous injury which can be troublesome source of bleeding. The tibioperoneal trunk down to the bifurcation and origin of the peroneal artery was exposed through the same incision. And anterior tibial artery origin was controlled with a vessel loop largely out of habit although it seemed clear it was occluded, as were the proximal popliteal and tibioperoneal trunk branches. The arteriotomy was created from the tibioperoneal trunk to the popliteal artery and endarterectomy was performed from distal to proximal to create a starting point for the ring dissectors used in remote endarterectomy. The anterior tibial plaque branched off much like an external carotid artery plaque and I decided to see what would happen if I did an eversion endarterectomy. I was able to mobilize a short length of the artery and was able to pull as I endarterectomized around the plaque and it thinned very nicely and came out with a gossamer end point. More gratifyingly, the backbleeding was excellent –this was controlled with the vessel loop very nicely. The retrograde popliteal endarterectomy was performed as described in another post in another case –link. The artery was then patched and completion arteriography was performed.


What was fascinating was it seemed I had reopened not just the pop-peroneal axis but the anterior tibial artery was also open, very dramatically so. The patient also had a bounding dorsalis pedis artery pulse. She recovered and went home two days later and in three years of followup while I was still in Iowa, she remained widely patent, maintained on Coumadin anticoagulation.
Popliteal endarterectomy for localized popliteal artery disease has been described (reference) with decent short term patency and successful limb salvage. Nasr et al. performed their endarterectomy via a posterior exposure. I think I recall coming across this in a book chapter from the old Wylie textbook which is long out of print. I think that the anterior tibial artery never lit up well because it was part of a highly developed collateral network, but it was patent all along. Duplex which was not done, would have given a better indication of its patency. I think that the patency of the popliteal endarterectomy is related to its relative shortness and in this case, the added outflow cannot hurt.
Reference
Nasr H et al. Popliteal endarterectomy for localized popliteal artery disease. Ann Vasc Surg 2014 (in press).

Dr. Gary Fass presented a decade long series of safe autograft harvest using SFA harvested for arterial bypass while reanastomosing remnant SFA to the PFA, achieving acceptable long term patency. This will definitely go into my armamentarium. Shows the poster sessions are often very useful!


Dr. Roberto Chiesa from Italy presented his experience in 61 renal arteries using the Gore hybrid graft today at the Veith Symposium The graft which I sketched above on my phone is their PTFE graft terminated in a Viabahn configuration. He reports a 10% acute renal failure rate and 90% primary patency in followup. This is something I’ve considered but never tried because the one extra anastomosis doesn’t add all that more time especially if a branched graft is used. Will revisit this concept.
Dr. Debus presented using this graft in a later talk for debranching visceral arteries in hybrid repair of TAAA.
