
The patient, a 47 year old woman, was referred for syncope, but it was much worse than that. Excessive stress, standing, and thinking hard were described as causes of her syncope. Frequent headaches and lethargy lead to inability to keep a job. Several MVA’s resulted in revocation of her driver’s license. Added to that was a two to three pack a day cigarette habit. Her cardiac workup was negative, but it was noted that her carotid duplex was notable for a left ICA occlusion and left vertebral occlusion. Blood pressure in both arms was in the 70’s systolic while in her better thigh it was 90’s. She had an open right carotid system but the flows in the common carotid were attenuated. CTA of the arch revealed severe arch disease affecting the origins of her great vessels. The innominate artery was severely diseased to its bifurcation with a small <2mm channel of flow. She had a dominant right vertebral artery that was patent, and the right ICA had moderate disease at its origin. This was in 2009, and I entertained intervention, but wasn’t all that confident that kissing stents into the innominate was all that great of an option even though there are reports of innominate interventions in the literature. I had the opportunity to perform a handful of great vessel reconstruction with Ken Cherry during my fellowship and felt that this was an ideal case for an innominate endarterectomy.
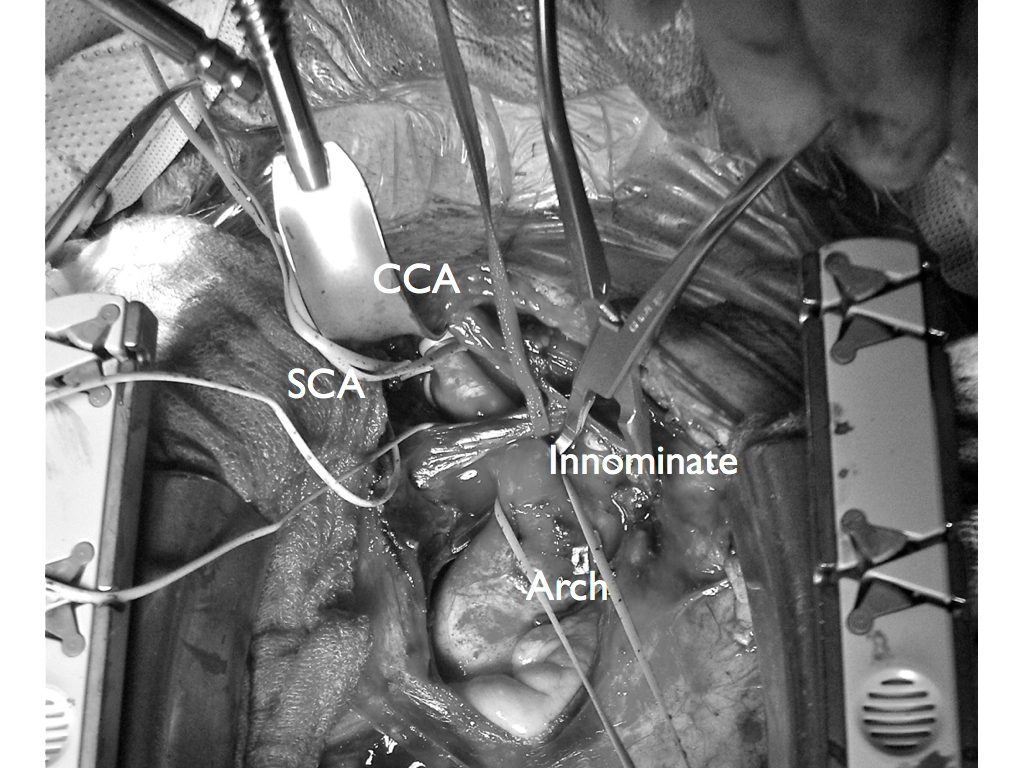
This is one of those rare and infrequent cases from vascular surgery history. The exposures is one of the grand vistas of vascular surgery. The arch, thankfully, was only calcified at the origins of the vessel and clamped well. The endarterectomy was not that much different from an aortoiliac endarterectomy with a fibrocalcific plaque and was extended onto the common carotid while the origin plaque of the subclavian was plucked cleanly. The phrenic and vagus nerves were protected. The patient was centrally hypertensive as found by a long femoral arterial line and was kept that way for the duration of the clamp. A bovine pericardial patch was applied and the sternum was closed over a mediastinal chest tube.
The recovery was impressive for the patient’s immediately improved state of consciousness, lack of lethargy, and improved cognition. She was herself impressed enough to quit smoking during that admission for good. Her right brachial cuff pressure now correlated well. She went home POD 5. When I last saw her 2 years later, she was employed and symptom free with continued patency of her repair, consistent with the earlier reports of this operation (Cherry et al. J Vasc Surg; 989;9:718-14).
