

At last week’s Veith Symposium, there was a straw poll for parallel grafts versus fenestrated stent grafts in emergent setting, and the results were a populist parallelist majority. This is clearly the result of years of inability to access this technology and reflects market forces making the decision over careful science. There are clear examples of this in the past -the adoption of laparoscopic cholecystectomy and appendectomy, done without randomized control trials shows that RCT’s be damned, people and surgeons will get what they want.
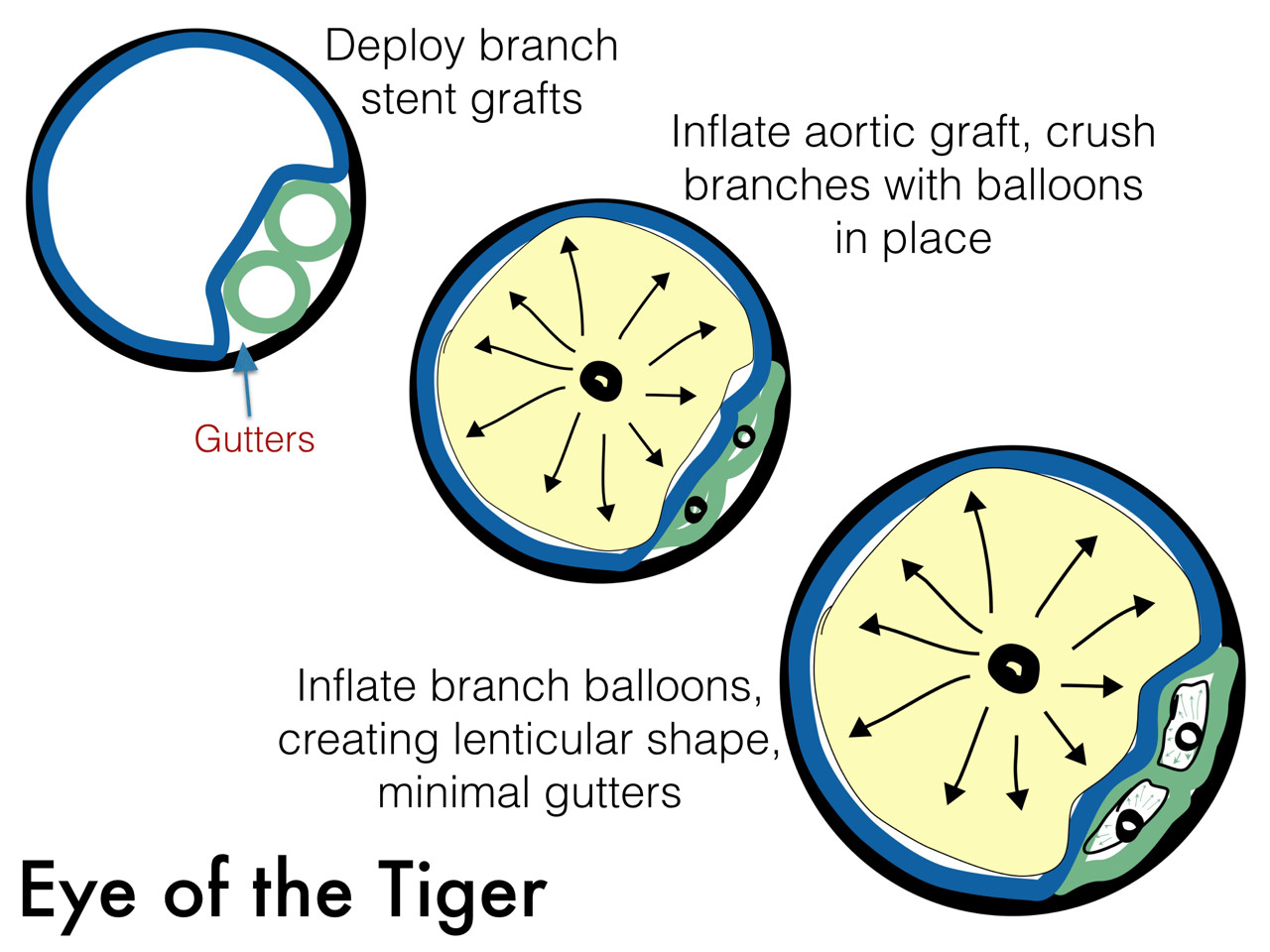
The several presentations on parallel grafts caught my eye. First was the Eye of the Tiger technique which sounds like a kung-fu move. Presented by Dr. David Minion of the University of Kentucky, the gist of it is that the gutters created by parallel grafts can be obviated by reshaping the branch grafts from circles to lenticular shapes (illustration). The sequence of moves is to deploy a balloon expandable stent graft outside of the main graft and deploy it, then deflate the balloon. The aortic graft is then ballooned, crushing the branch graft. With the balloon inflated, the branch graft is then inflated, now taking a lenticular configuration. This, I will put in my tool box.

The other presentation was on the bullfrog catheter, by Dr. Christopher Owen of UCSF. It inflates to press the catheter portion of it in the middle of the length of the balloon against the stent graft wall. A penetrating needle then comes out through the graft material, allowing for infusion of a sealing embolic material. This has not been tried in humans but application in an animal model is ongoing.

I have a feeling parallel grafts will be with us for a while. Using these in conjunction with the Nellix graft, juxtarenal aortic aneurysms were treated, which brings me to think that with the inevitable progression of paravisceral segment aneurysm disease, we will be seeing secondary endobags (not a pejorative) for treatment of paravisceral aortic aneurysms with parallel grafts, and we will see something like this on CT scans one day (illustration). Mr. Ian Loftus of St. George’s Vascular Institute reported on 19 patients (11 single, 5 double, 3 triple branch) over 12 months who were unsuitable for OR/EVAR solutions, treated with 100% technical success, one type I endoleak. Dr. Michel Reijnen presented the Arnhem experience with this technique. Their series included 7 patients with juxta (5) or para (2) renal AAA’s (4 single, 2 double). He reported 100% chimney graft patency and no reinterventions in short followup. He presented a case of rupture, but warned that further investigation would be needed before using the endobag for rAAA.
I think that the whole issue points to several truths. Paravisceral and thoracoabdominal aortic aneurysms have always been viewed with trepidation and this generally caused referral of these cases to high volume centers and surgeons during the open era. Experience with EVAR has infused a sense of confidence and with mastery of infrarenal EVAR and basic endovascular interventions, most practitioners feel ready to offer an endovascular solution to the visceral segment AAA’s, but feel locked out either through lack of training or inability to access the devices, particularly not having ready solutions on the shelf. These parallel graft systems offer relative ease of delivery and use readily available components. Even I have resorted to parallel grafts in an emergency with acceptable short term result (patient lived) but with uncertainty with durability.
I think that there will never be a completely satisfactory off the shelf, “every-surgeon” solution because these patients are no less complex when approached with endovascular technique -they just present a different set of equally difficult challenges. As in open repair of these complex aortic aneurysms, endovascular repair of these should aggregate to high volume practices and centers with deep experience.
