Sketch of Dr. Gilbert Upchurch’s hybrid treatment of TAAA, at least as I understood it.
The VEITH Symposium has been my favorite meeting since I was a junior resident back in the 90’s. This year is no different. I finally figured out why I like it so. VEITH is organized like the Iowa State Fair with all the charms and chaos that makes that fair one of the top 10 things to do in the US. There is the location at the Hilton Midtown which puts it in the center of all the commercial and tourist chaos that makes NY amazing. It is a high end version of the midway at the Iowa State Fair on East Side night, but instead of fried Snickers and bad teeth, you have perfectly crafted international foods and people from everywhere. Like the Iowa State Fair, everything is happening at the same time and you have to plan out your day in great detail. And there are the must sees like the debates between the giants of the field and the 20 surgeon panels sitting on stage no different from the 1000 pound pig and the handsomest cow. Then there is industry, but rather than tractors in green or blue flavors, we get seven different kinds of stent grafts at my last count. You learn how to pick out the signal from the noise, not always by counting the N of individual papers, but in the trends of the numbers of presentations that generally agree, like the hot new Fair food that catches and gets easier to buy every subsequent year. A true free market of ideas. And finally, like you can run into friends who moved to Dubuque, you run into people who were important on your life path, Jedi and Sith masters and padawans, and you have large unhealthy dinners together. What’s not to like? Next year, at VEITH!
Why perform such an extensive endarterectomy when just a few stents will do? This is a valid question, given the relative safety of interventions and the durability of bypasses. There are three reasons why ilio-femoral-popliteal endarterectomy works well in my practice.
Minimally invasive
Restore elasticity and collaterals
Move the inflow point from the groin to the knee
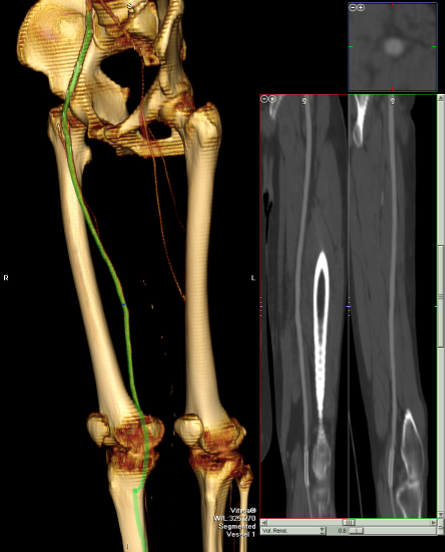
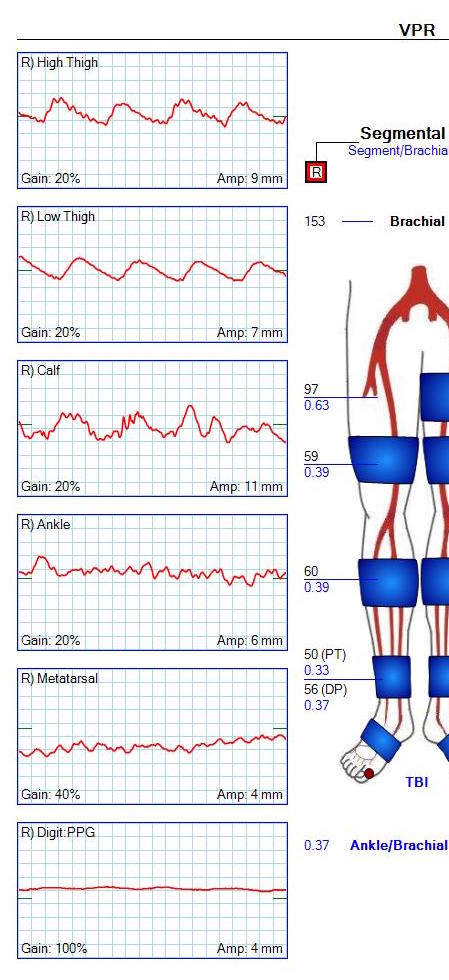
The procedure is minimally invasive. Take for example this patient whose plaque is shown above. He had a common femoral occlusion for which a common femoral endarterectomy was aborted when the prior surgeon ran into excessive bleeding. Workup for coagulopathy was negative and the patient came to me with rest pain. Pedal level pulses were not palpable, and the signals were barely there.
CTA showed that he had a CFA occlusion as well as SFA occlusion.
Because the common femoral plaque is contiguous with the external iliac plaque, it is often simpler to complete a remote endarterectomy over wire up to the external iliac origin than to try to get a satisfactory end point at the inguinal ligament -I do not like stenting across the ligament into the patch which is the usual bailout if the end point causes a stenosis. It is far simpler to apply a stent at the external iliac origin.
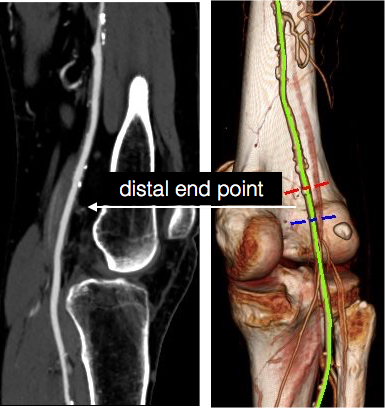
The popliteal end point was chosen where the visible plaque was no longer apparent in the patent artery. The goal is to cut across thin intima, and frequently no distal stent is required because a secure end point is achieved much like the “feathered endpoint” seen in carotid endarterectomies.
My intention was to endarterectomize the atherosclerotic plaque from the external iliac origin to popliteal artery via the groin incision marked in orange.
3DVR allows for planning the operation in great detail
The video shows the setup and motion in dissecting the plaque.
The plaque came out easily (first image, top).The proximal and distal end points required stents.
Before and after
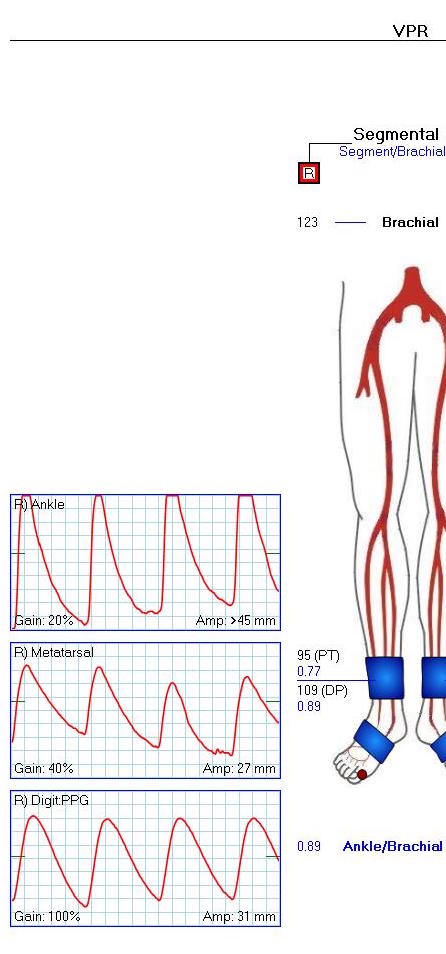
The patient regained palpable dorsalis pedis and posterior tibial artery pulses. Total OR time was less than 2 hours. An ilioinguinal field block allowed for good pain control and the patient was discharged the next morning, having to heal only a 10cm wound. There is no good endovascular option for common femoral disease, and while stenting the whole SFA can be done, on more than a few occasions I have had to treat occluded “full metal jacket” SFA stents, usually by removing them. EndoRE has been shown to be superior to PTFE and almost as good as vein in the REVAS Trial when compared to fem-AK POP bypass. Going home the next day after such an extensive revascularization is not a stunt -it’s the direct result of limiting the incision and blood loss and OR time.
2. Restore Elasticity and Collaterals -Arterial Restoration
One of the components of arterial flow that is lost with atherosclerotic disease is arterial elasticity. That is the stretchiness of the artery in response to pressure. Elastic distension and recoil account for significant portions of forward flow during diastole which is lost with atherosclerotic plaque. As plaque builds up, and the artery becomes stiffer. The artery that goes through remote endarterectomy regains this elasticity. Ultrastructure from a recanalized external iliac artery sampled from a punch arteriotomy for a cross ilio-femoral bypass showed that three months after endarterectomy, the external iliac artery was ultrastructurally normal per pathology report.
Also, collaterals that were previously occluded are seen to be restored to patency. This has an important impact on patency and any future failures. The endarterectomized arteries fail due to the presence of isolated, random fragments of medial smooth muscle which cause focal TASC A restenoses. These are easily amenable to balloon angioplasty. If the revascularization fails, there is no catastrophic thromboembolism that is typical of PTFE thromboses -rather the collaterals keep segments open and it is straightforward to thrombectomize or lyse the artery and intervene as necessary.
3. Moving the inflow point from groin to the knee.
This is an important concept. One of the principles of inflow restoration is delivering large flow and pressure directly from the aortic source to the leg. Recanalizing from the external iliac to the below knee popliteal artery creates this situation below the knee, allowing for very short bypasses to be performed from the popltieal artery to tibial targets -a very useful circumstance when vein is limited. This next patient is a presented with gangrene of his fifth toe after esophagectomy for cancer, and had severe diabetes.
He had useful saphenous vein in his thigh only, some of it having been harvested in the proximal thigh for a common femoral endarterectomy. CTA showed a dilated common femoral and profunda femoral artery, severely calcified SFA and popliteal artery which were occluded, and only a patent peroneal artery as runoff.
The plan was to harvest the short segment of vein then through the same incisions, below the knee and in the mid thigh, expose the below knee popliteal artery and tibial origins, and the mid SFA. I intended to avoid the groin. The plaque was removed from the tibioperoneal trunk to the SFA origin, and the origin was stented.
This reestablished a normal inflow at the level of the below knee popliteal artery. I also did an eversion endarterectomy of the anterior tibial artery which resulted in significant back bleeding -a good sign. A short bypass was performed from the below knee popliteal artery to the peroneal artery.
This resulted in a palpable dorsalis pedis artery pulse and excellent peroneal and posterior tibial artery signal.
The ABI improved and the waveforms predicted healing for his 5th ray amp.
This last case illustrates the point that once the conceptual inflow point is moved to the below knee popliteal artery, bypasses can become short, and durable tibial revascularizations become feasible. By avoiding a redo groin, avoiding multisegment arm vein bypass, and keeping the procedure time under 5 hours, the operation remains less invasive.
The dictum that better is the enemy of good is one of the old chestnuts carried around surgery training forever. It is an admonition against an unhealthy perfectionism that arises from either vanity or self doubt, and in the worse cases, both. The typical scenario is a surgeon trying to make a textbook picture perfect result and finding the patient’s tissues lacking, will take down their work to make it better, and repeat this process while the patient and everyone else in the room lingers.
Trying to avoid this, many surgeons will try to avoid any difficulties -the bad patch of scar tissue, irradiated body parts, areas of prior infection. But the mental contortions involved in avoiding “perfect” can result in actual physical contortions that in the end don’t pay off in good enough. I have not been immune to this, and I don’t think any physician or surgeon can honestly say they haven’t experienced some variation on this.
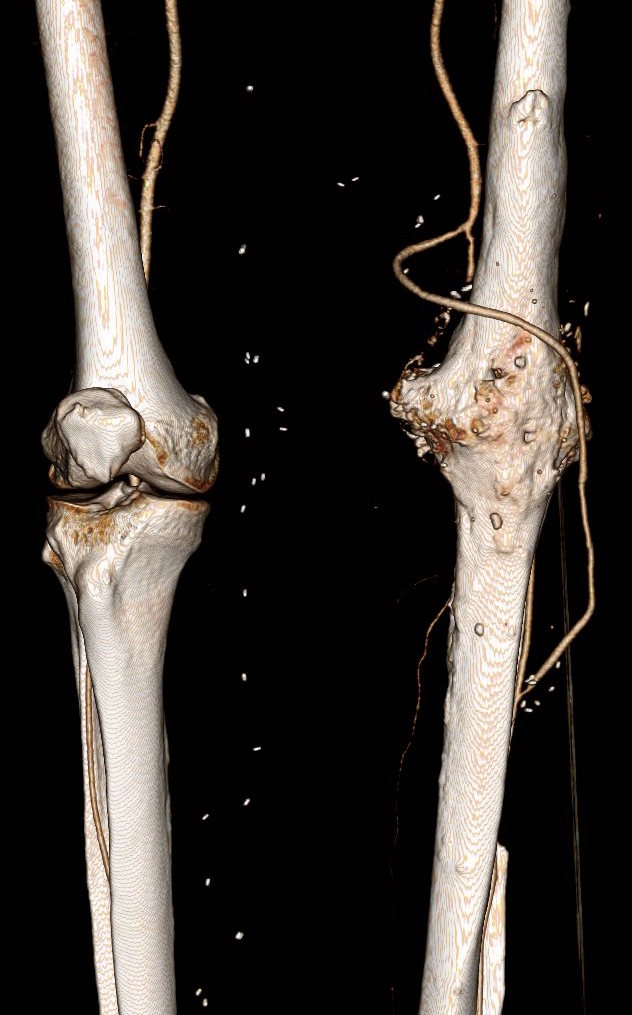
This patient is a younger middle aged man who in his youth experienced a posterior dislocation of his left knee, resulting in an arterial transection. This was repaired with an in-situ graft. Subsequently, he had complications of osteomyelitis and had his knee fused after resection of his joint. He did well with this bypass for several decades, but it finally failed several years ago, and a new one was created (image above).
Rather than directing the graft in line as in the previous one, this was was taken from a medial exposure of the femoral artery and tunneled superficially around the fused knee to coil lateral, ending in the anterior tibial artery.
This graft in turn thrombosed and was lysed by the outside surgeons and underwent serial interventions of proximal and distal stenoses at the anastomoses. The patient, when I met him, was contemplating an above knee amputation as a path to returning to work as a nurse in a rural hospital.
While there should be no reason long bypasses should do any less better than short bypasses, I do have to say these things about this patient’s bypass:
No vein is perfect and the longer your bypass, the more chances you will have that a segment of bad vein will end up in your bypass
Turning flow sharply can cause harsh turbulence. Turbulence can cause transition of potential energy into kinetic energy which acts to damage intimal, resulting in intimal hyperplasia.
Thrombosis is a sure sign that your graft is disadvantaged, and the longer the period of thrombosis, the longer the intima “cooks” in the inflammatory response that accompanies thrombosis, making the vein graft even more vulnerable to subsequent intimal hyperplasia, thrombosis, or stricture.
A high flow, small diameter vein graft entering a larger, disease free bed results in more turbulence but also Bernoulli effects that cause the graft to close intermittently, vibrating like one of those party favors that make a Bronx Cheer (a Heimlich valve). This is the cause I think of the distal long segment narrowing on this graft.
This patient was decided on amputation when our service was consulted, and after reviewing his CTA, I offered balloon angioplasty as his symptoms were primarily of paresthesia and neuropathic pain. I used cutting balloons and got angiographically satisfactory results.
The patient, although he admitted to feeling much better, was sad. He relayed that he had felt this way several times before, only to have his life interrupted by pain and weakness signaling a restenosis.
A direct graft would require about 10 centimeters of vein
It was only a month later when I heard the patient had returned with the same symptoms. He wasn’t angry nor full of any “I told you so” that frankly I was muttering to myself. Reviewing his CTA, he had restenosed to a pinhole. The vein, to use a scientific term, was “no good.”
The other interesting finding was that he had an abundance of very good vein. Following surgical dictum, his original and subsequent surgeons had used his vein from his contralateral saphenous vein. His right leg, fused at the knee, lacked a good calf muscle pump action. While there were no varicose veins, the greater and lesser saphenous veins were large and generous conduits, at least by 3DVR imagery, confirmed on duplex (image below, white arrows).
3DVR showing presence of potential conduit
The extant arteries were smooth and plaque-free. I decided to harvest his lesser saphenous vein and through the same incision expose his distal superficial femoral artery and tibioperoneal trunk. While I anticipated some scarring, I was confident that the sections of artery I wanted to expose were easy to access because of some distance from the fused knee.
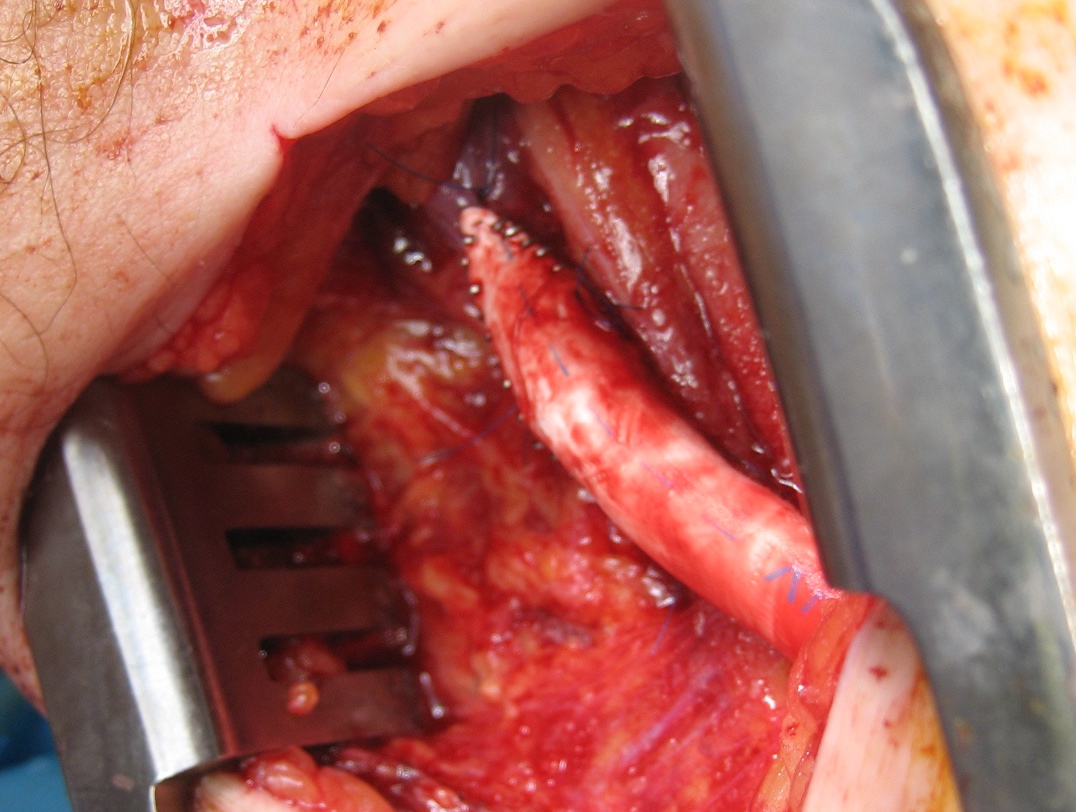
On left short saphenous vein was harvested then same exposure used to expose TP Trunk
The picture shows the exposure and reversed vein graft in-situ, using the segment of lesser saphenous vein. As in prior experience in redo surgery, you can never know if a dissection will be easy or hard simply based on fear or concern for breaking something. It’s not until you start bushwacking –carving through scar and dealing with extraneous bleeding will you learn whether it was easy or hard. You can only be certain it was necessary. The only hitch was the femoral artery while well exposed, was buried in scar, and I chose not to get circumferential control as I was fairly deep, and had avid backbleeding from a posteriorly oriented collateral that required a mass clamp of the deep tissues.
Will this work better? Don’t know but it has a good chance, and I think a better chance. It is a large vein oriented in a straight path over a short distance going from good artery to good artery. This is better theoretically than a long meandering bypass with smaller vein.
The patient, a younger middle aged woman, was referred for treatment of a large, growing infrarenal AAA over 8cm in size complicating a severe pancreatitis. The pancreatitis occurred about a month prior to presentation and resulted in a substantial pancreatic leak. At the time of that presentation, her AAA was found incidentally and was about 7cm. In the interval, her pain resolved and she was asymptomatic. On examination, her abdomen was soft, and a large aortic aneurysm was easily palpable.
Pancreatitis with surrounding retroperitoneal fluid leak
CT scan was performed showing an enlarging AAA over 8am and abundant retroperitoneal pancreatic fluid without abscess or infection. The AAA was infrarenal but complicated by a severely tortuous, short infrarenal neck with 90 degrees of angulation and about 8mm in length. As the pancreatic leak was yet early in the process, no pseudo aneurysms had formed. MRCP showed no active leak.
Short neckGreater than 90 degree neck angulation
Other than the pancreatitis, the patient, who was in her 50’s, was an otherwise good risk patient.
The treatment options were:
1. Wait until pancreatic fluid resolution or pseudo aneurysm formation, then standard open repair of the large aortoiliac arterial aneurysm. Not desirable because of the relatively rapid aneurysm growth and current size.
2. EVAR -This is outside the IFU for any of the available devices because of the highly tortuous neck anatomy. While note shown, the external iliac arteries were 5mm in diameter, but in the absence of plaque, was possibly due to spasm. The Nellix device is yet on trial, but there are limits on how much you can straighten this neck. The devices with suprarenal stents end up straightening out the graft with deployment of the graft in an ellipse. This also means loss of seal zone length which decreases with oblique deployment. FEVAR is not possible because of this neck tortuosity as well but was considered briefly.
3. Homograft repair or Rifampin soaked graft repair -The former is costly and still susceptible to infection from a virulent organism as is the latter, but both are likely safe with likely foregut flora.
4. Neo-Aorta reconstruction (NAS) with deep femoral vein. This could work, but is time consuming and relatively morbid. The tactic of mobilizing the vein and then repairing the aneurysm in a separate, staged fashion the following day or two is reported to shorten the overall operative time. This patient would require both femoral veins to be harvested.
5. Aneurysm exclusion and extra-anatomic bypass with axillofemoral bypass. Offered to complete this list, this is the least desirable option given the poor long term behavior of axillofemoral bypasses in younger patients.
When faced with this kind of challenge, it makes sense and should be standard practice to get the opinion of the group. I happen to have excellent partners to run this kind of cases. The consensus was this: EVAR with accepting a short term result to temporize until definitive repair could be done. I found this acceptable. I chose to use the Excluder device because it allows for redos of the proximal deployment (C3 Delivery system) and the 23mm and 26mm devices used 16F access. A detailed discussion with the patient and the intention to eventually definitively repair open was discussed and patient was agreeable to proceeding. Plan B’s of Rifampin soaked graft replacement and NAS was also discussed.
I tried two things that was different. I felt that a stiff wire would result in horizontal orientation of the top of the graft, and so I placed a bend in the wire. Prior experience with unintended bends in wires have taught me that passing these wires is largely tolerated as long as it is done through catheters and sheaths. The other thing I did was bend the top of the delivery system -this was done with some care as I did not want to detach the contraining mechanism.
The wire and delivery system modification did tilt the top of the graft away from the left side of the aorta. It had the unintended effect of keeping the wall grabbing anchors away from the near wall while constrained.
It didn’t tilt the graft as much as I would have liked, but the graft deployed in a left to right fashion that allowed for controlled delivery across all of the available neck. Gratifyingly there was seal (below). I flared the right, while excluding the left iliac bifurcation because of the larger iliac aneurysm.
As this was done percutaneously, the patient recovered rapidly and was discharged a day later. The question philosophically for me is if the seal remains intact, would there ever be a need for explantation? The patient only received perioperative antibiotics, and I felt long term antibiotics was not indicated. Standard followup was arranged.
There is no question there is a need for devices designed for this kind of neck anatomy. These devices need to bend over to angles at least 90 degrees and unbend based on delivery system design. They need to be low profile as this facilitated repair in this patient with small access vessels.
update:
After she recovered, her interesting case was published as a case report in BMJ:
Karam PA, Moslim MA, Park WM, Morris-Stiff G. Abdominal aortic aneurysm in the setting of Clostridium perfringens pancreatitis. BMJ Case Rep. 2017 Aug 7;2017:bcr2016218549. doi: 10.1136/bcr-2016-218549. PMID: 28790092; PMCID: PMC5612546.
The ligamentum arteriosum, the remnant of the ductus arteriosus between the aortic arch, tethers the arch causing a tear during sudden deceleration like hitting a steering wheel with your chest
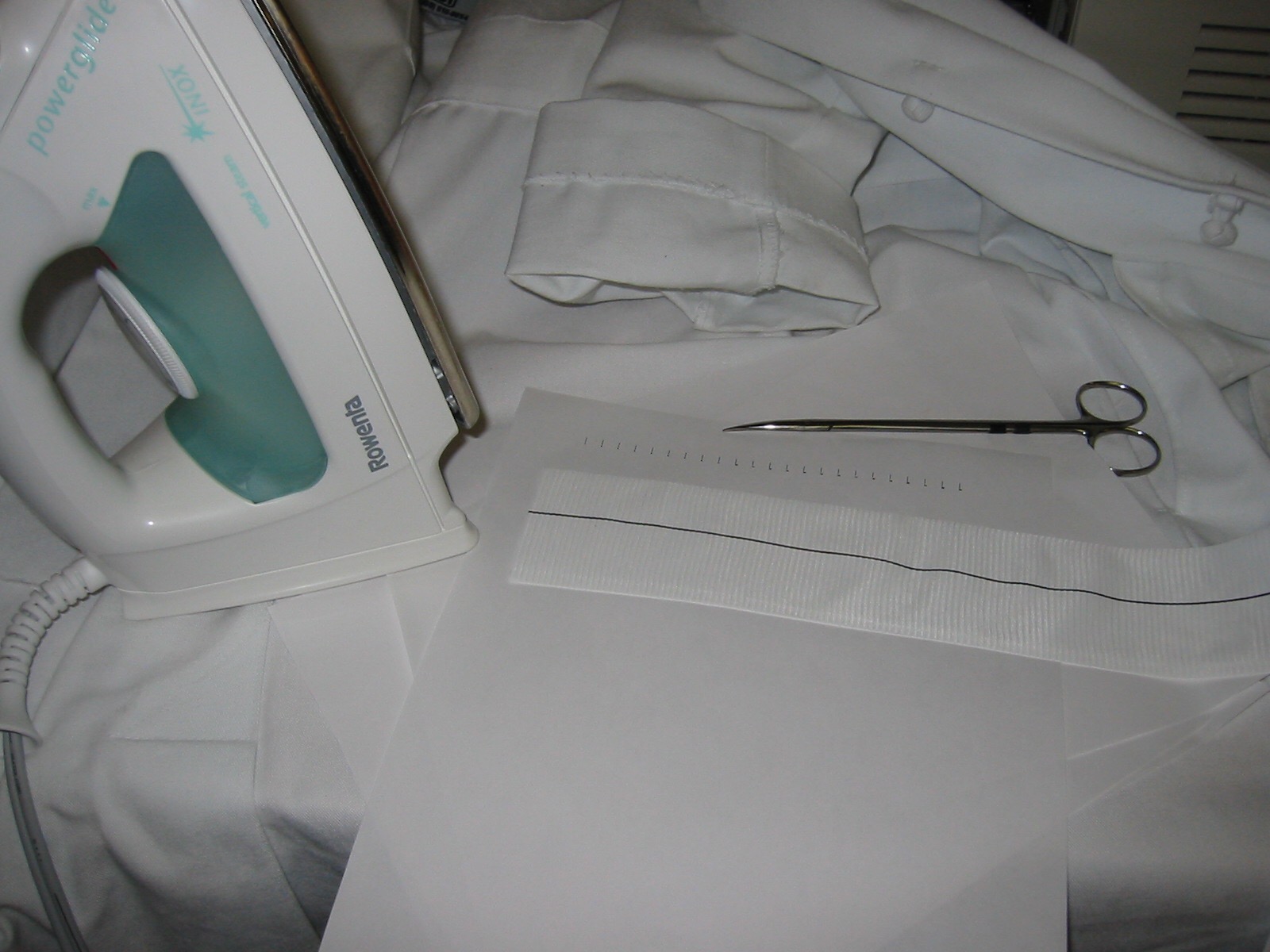
I recently repaired a traumatic aortic dissection and was struck by how far along things had progressed since I was a resident. I remember seeing a Q&A in the mid nineties where Dr. Mattox expounded on the gold standard for diagnosing traumatic aortic injuries which at that time was contrast aortography. This caused many struggles trying to arrange for arteriography in the middle of the night (these accidents usually occur then). The repairs were open and very morbid for severely injured patients, particularly those with closed head injuries and fractures. This all changed in the early 2000’s as I had mentioned in an earlier post (link). The grafts were homemade (figure)
and this was literal -the picture is from my kitchen back in the Bronx in 2004. The grafts were cumbersome to deploy and required long 24-28F sheaths that frequently required iliac and aortic exposures.
The revolutionary breakthrough was the fact that thoracotomy and partial cardiac bypass could be avoided. Durability was largely assumed as these patients rarely came back for followup.
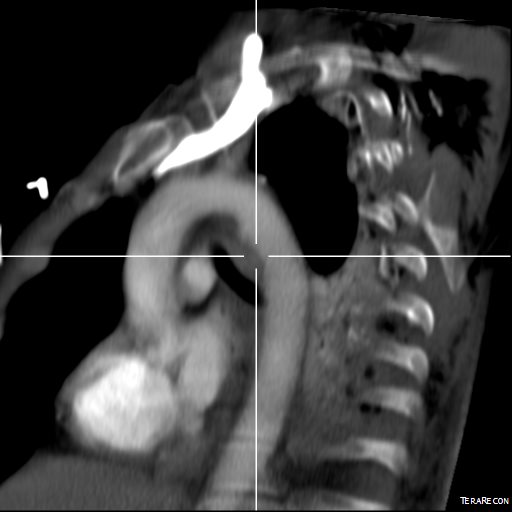
Fastforward to 2015. CTA is done with 64 slice CT scanner with EKG and respiratory gating eliminating the artifacts that caused Dr. Mattox to assert that aortography was the gold standard. Software based image reconstruction can aid treatment planning in ways that greatly exceed the caliper and ruler methods we had in 2004.
The grafts are currently into their second generation of development and have small profile and trackability that allows for percutaneous delivery and treatment.
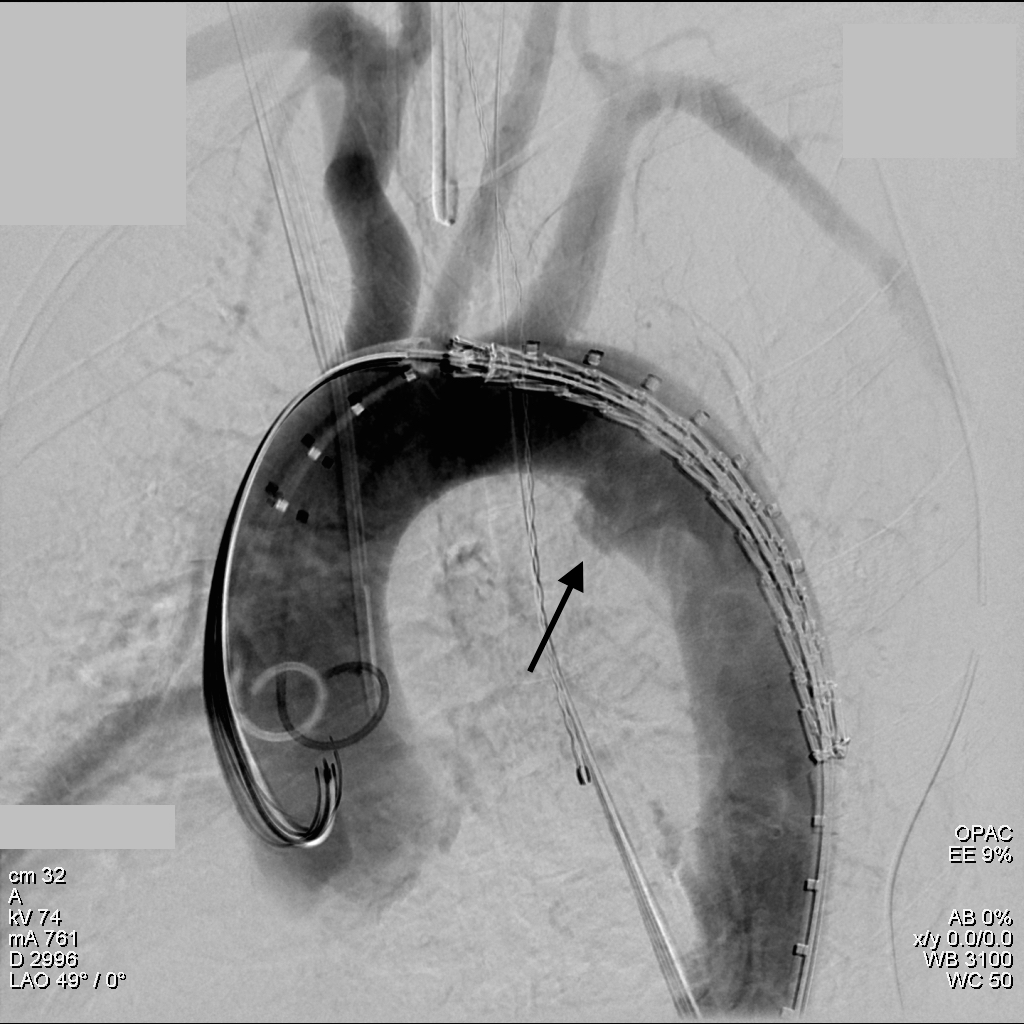
The aortogram shows the tear along the inner curve. These lesions typically require coverage either partial or total of the left subclavian artery origin. This patient had a dominant right vertebral artery and I felt he would tolerate even full coverage of the left subclavian.
The device, a Gore C-TAG device which has an FDA trauma indication, is clearly better than our homemade device. Deployment does not require pharmacologic or electrical bradycardia or asystole.
The idea behind this design is conformability of the smaller stent elements. The aortic injury is even outlined by the stents in the aortogram above. The bird-beaking that was common to the prior generation of graft is not seen in this aortogram.
Where does this need to go next? At 18-24F access requirements need to become 12-18F and for the same reason, the grafts need to be available down to 14-18mm as trauma doesn’t just happen in middle aged men. Aside from that, it is a definite improvement over what we had in 1995 and in 2004.
The picture above shows a vascular anastomosis created by an ingenious gadget that has struggled to find a place in my personal kit despite performing well. It really works well when you don’t have an assistant to follow your running suture to apply tension and keep the suture out of the way. I have have come up with four reasons why I don’t use it every day even though I like the device, find it performs well, and have used it in the past.
1. Training Vascular Surgeons- The vascular anastomosis is over a century old, and the various forms it takes, interrupted suture, continuous, end to side, end to end, side to side, native to prosthetic and so on, all have to be taught so that the trainee can function even in the absence of such gadgets.
2. Cost- The cost of the device is subsumed by the hospital and ultimately the healthcare system. Using the device is the equivalent of turning the air-conditioning on when opening the window will do.
3. Time savings- If operating room time were metered like taxi time, then there might be an argument for this device, but the difference in the end is still trivial. A hand sewn anastomosis, even done slowly, takes usually no more than 20 minutes. Using this device, the times are reduced to about 1-5 minutes. This almost never is enough to make a difference, unless ischemia sensitive tissues are being repaired, but no one would use this device to sew a graft to a renal artery.
4. Results- The argument that an interrupted anastomosis is superior to a running one only works when native tissues are sewn to native tissues. A prosthetic to artery anastomosis will not adapt and frankly is the easiest to create a technically acceptable anastomosis with. An interrupted anastomosis done by hand can be done in as much time as a running one (figure below).
There are many wonderful and ingenious inventions like this. Whole specialties and institutes are built around implantation of ingenious and life saving devices. Yet the costs are increasingly astronomical and unsustainable.
Can there be innovation without sticker shock? The answer is a qualified yes. To make this a reality, there has to be several changes in the way that devices and procedures are vetted and approved. It will not be easy.
To bring a new drug to the market, the Tufts Center for the Study of Drug Development estimates in 2014 that it costs $2.5 Billion. This barrier which we have erected against ourselves insures that pharmaceutical development is channeled through a narrow group of players. On the device side, there are similar barriers and price tags to bringing a discovery to market. There is a six letter C-word to describe this situation, but it isn’t polite to use.
It used to be that breakthroughs in surgery were not directly monetizable. The carotid endarterectomy didn’t make DeBakey or Eastcott anything but fame among a small group of surgeons, but there was great good from that. A lot of time and effort and money has been used in an effort to supplant the carotid endarterectomy with carotid stenting, but the devices come at a greater cost for dubious benefit except in very particular situations. I recently performed an eversion carotid endarterectomy in about an hour’s time closing with no patch or shunt. The procedure cost the price of 6-0 suture to repair the artery, and several packs of an absorbable suture to close the skin. Add to this some disposable drapes, suction tubing, a cautery and an energy device. Compare this to a carotid stent procedure that uses a stent (4 figures), wires (up to 4 figures), protection device (4 figures), sheaths, balloons and catheters (3-4 figures), resulting in upwards of 5 figures of cost. This is for a procedure that in head to head comparisons results in a higher stroke rate, the very complication it is meant to prevent.
Health care innovation will have to have cost disruption as a necessary condition for its adoption. Whatever is used, has to drop the cost by removing a zero from the end of the price tag while yielding at least as good or better results.
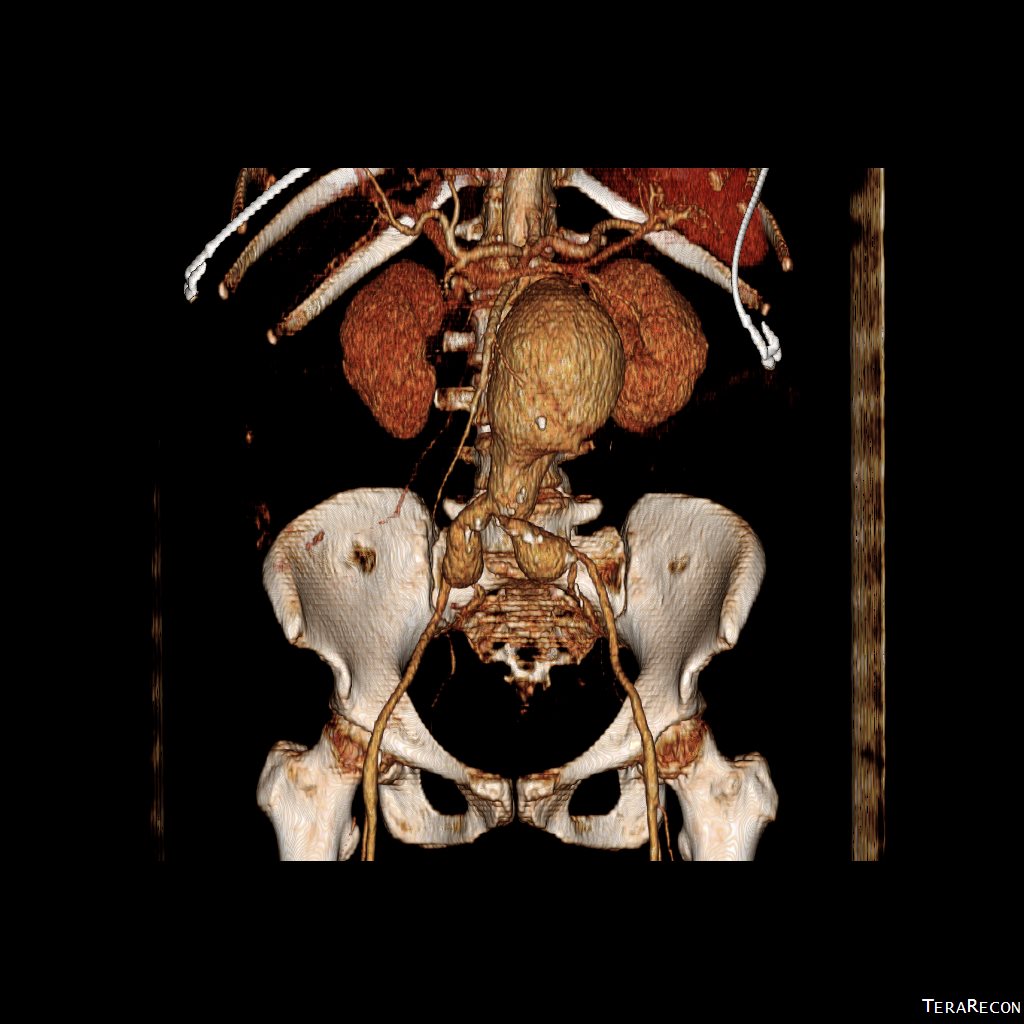
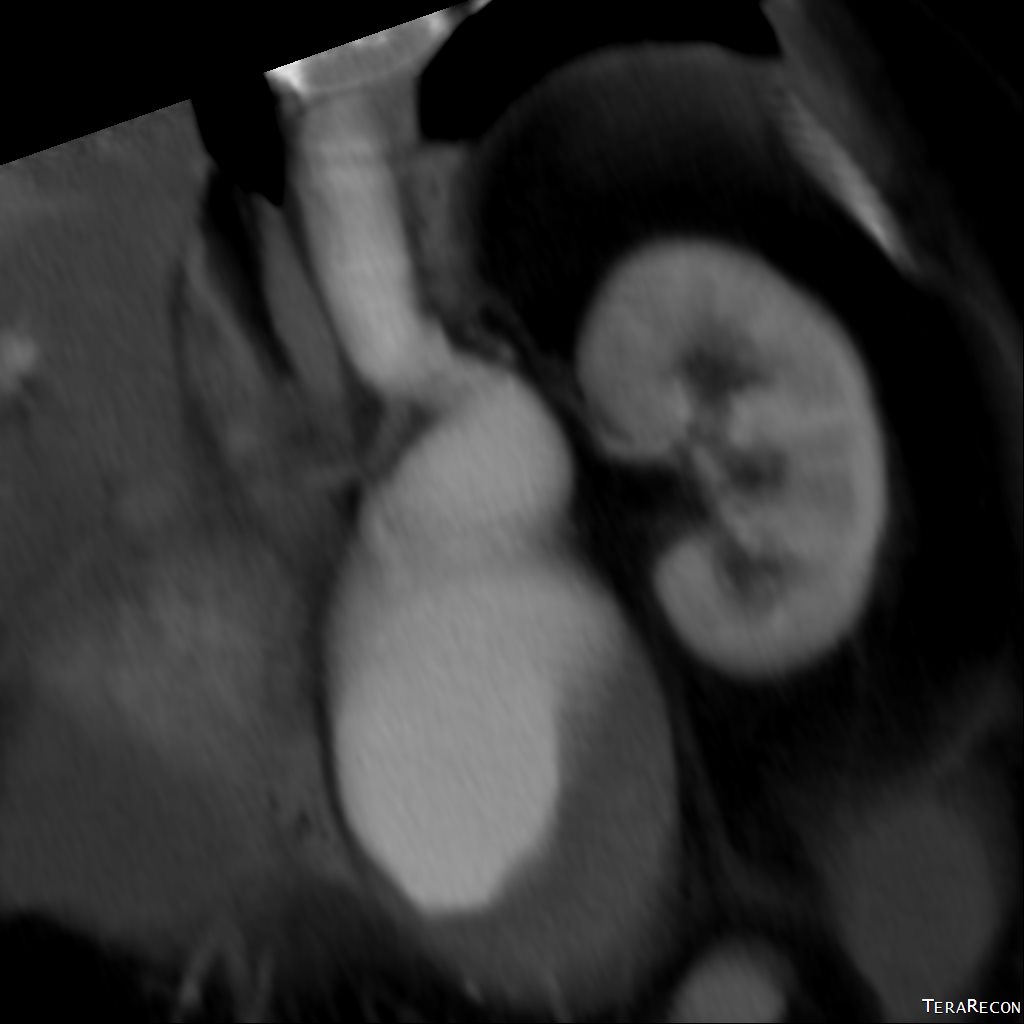
The patient had a carotid dissection over five years prior to presentation and had a stroke and DVT. To protect her from pulmonary embolism, an IVC filter was placed, she was anticoagulated for a while. She rehabilitated and was doing well when several months prior to consultation she developed severe upper abdominal pain that occurred intermittently without triggers. She underwent a workup which included laboratory testing and endoscopy which were negative, and a CT scan showing the IVC filter had tilted and the legs had eroded through the vena cava to abut the duodenum and abdominal aorta. No other pathology could be found and after discussion operative resection was planned.
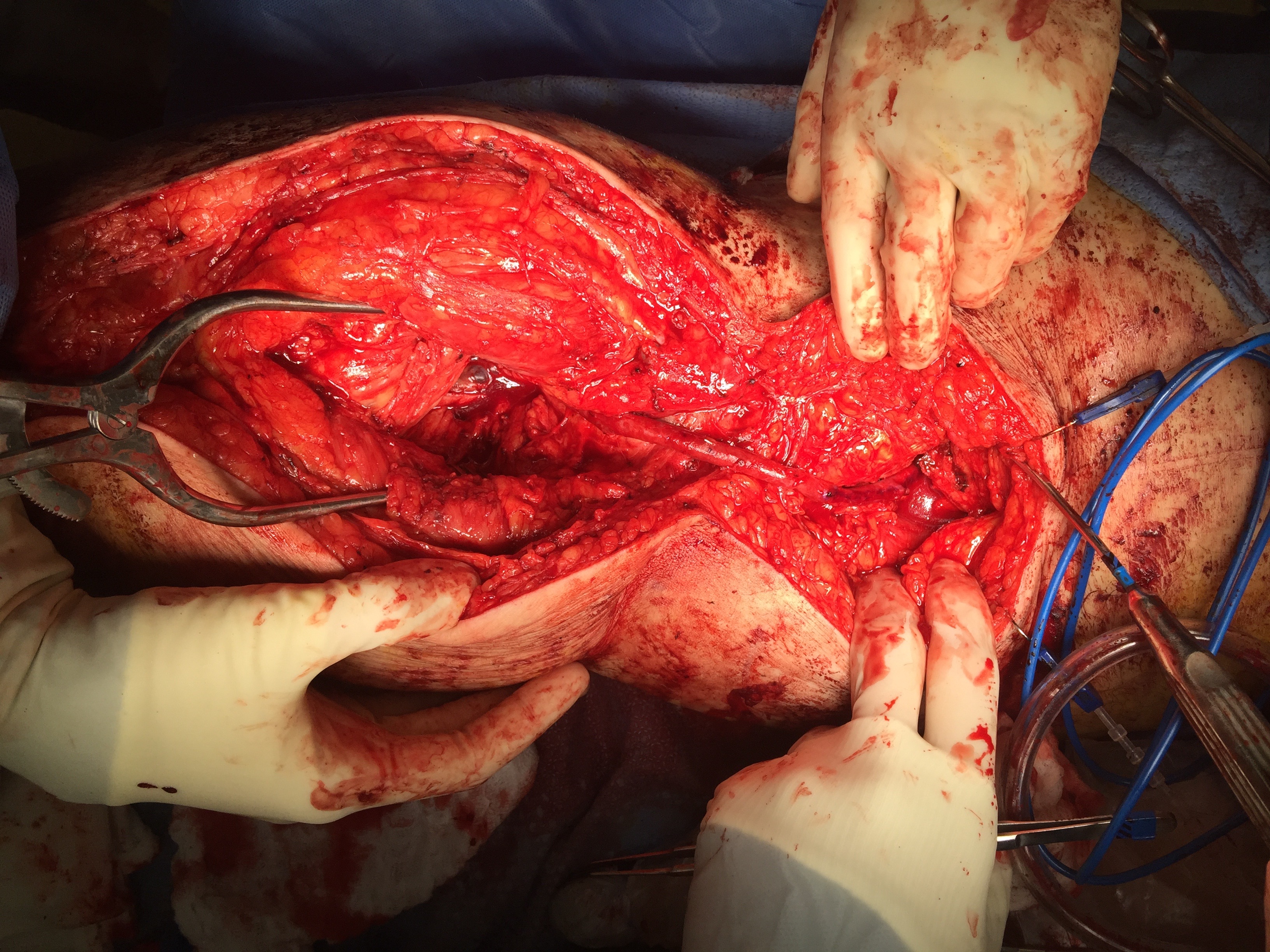
As mentioned in an earlier post, 3DVR image processing has become indispensable in planning not only aortic interventions but open surgery as well. An oblique incision was created, basically a high transplant incision, and we stayed in the retroperitoneum. The leg of the filter abutting the duodenum did not penetrate it and there was no leakage of bile. The end of the leg, of which there are two types on this filter, was in the vena cava, but the side had eroded out of the cava. Control of the IVC is always treacherous because of the fragile lumbar tributaries underneath the cava. Once heparinized and clamped, a longitudinal venotomy released the filter. The head was embedded in the cava wall and would not have been easily accessible with a snare.
The tine that was headed towards the aorta had to be removed from the filter to manipulate it out. No bleeding was noted from the aorta.
This is my fifth operative removal of an IVC filter that had eroded into adjacent organs. Recently I removed a filter which had eroded into the aorta -this required a pledgetted suture. In my first case, about 7 years ago, a filter placed in a teen, the victim of polytrauma due to an MVA, caused fevers and an upper GI hemorrhage which was diagnosed on upper endoscopy -somewhere I have a great picture of an IVC filter leg in the duodenum.
Which brings me to my last point. The guidelines for placing these filters has evolved and it is clear now that they are not as benign as once thought. They are not only associated with migration but also iliocaval thrombosis. Stenting across them can push the legs out into organs. Their migration into the retroperitoneum can cause an atypical abdominal pain syndrome -in this patient, the pain was immediately gone. If placed, plan should be made for removal if feasible, anticoagulation maintained if possible, and filter choice limited to those that have long track records.
The treatment of venous thromboembolism remains primarily pharmacologic. When the indication for the filter expires, the filter should be removed unless the risks of removal exceed the risks of leaving it in.
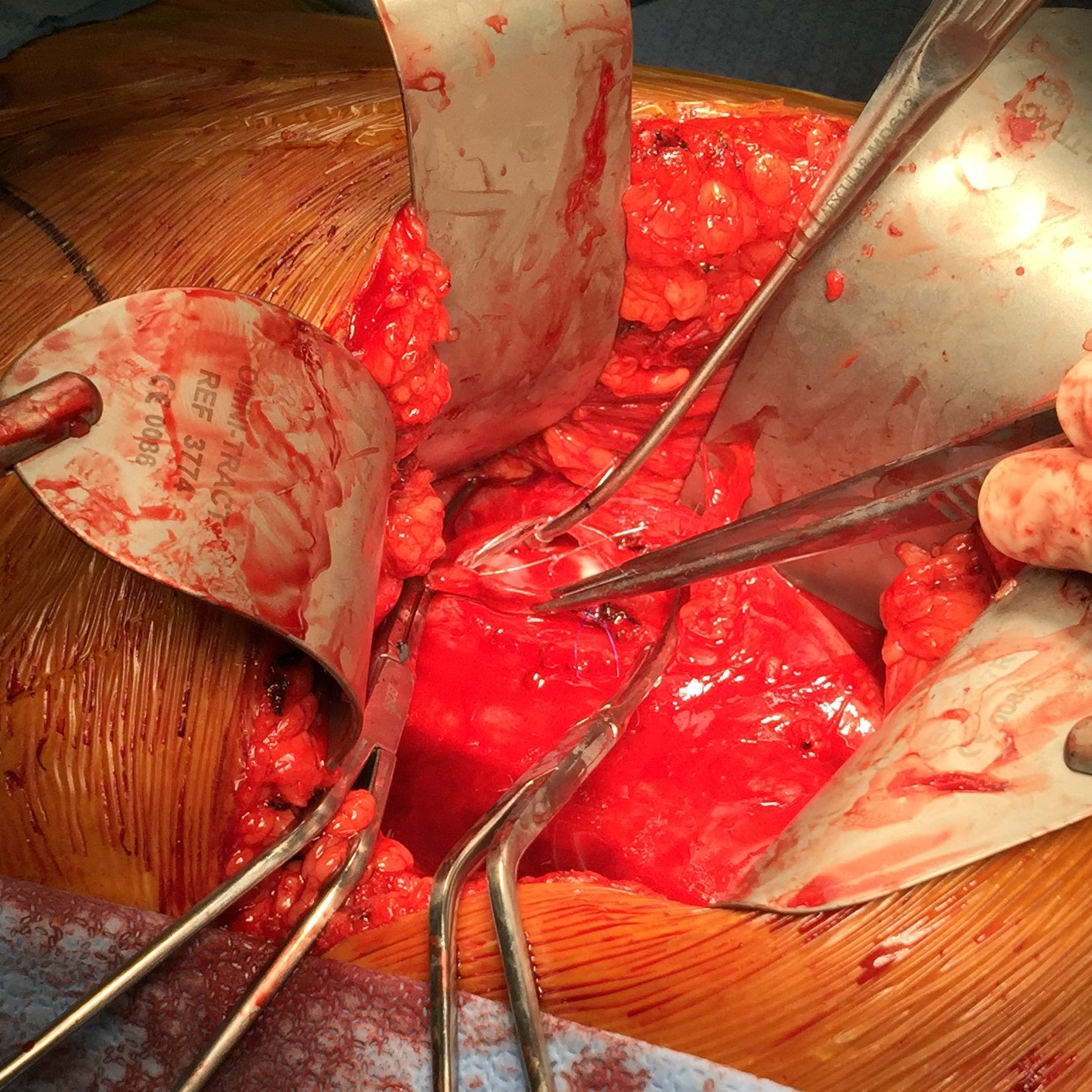
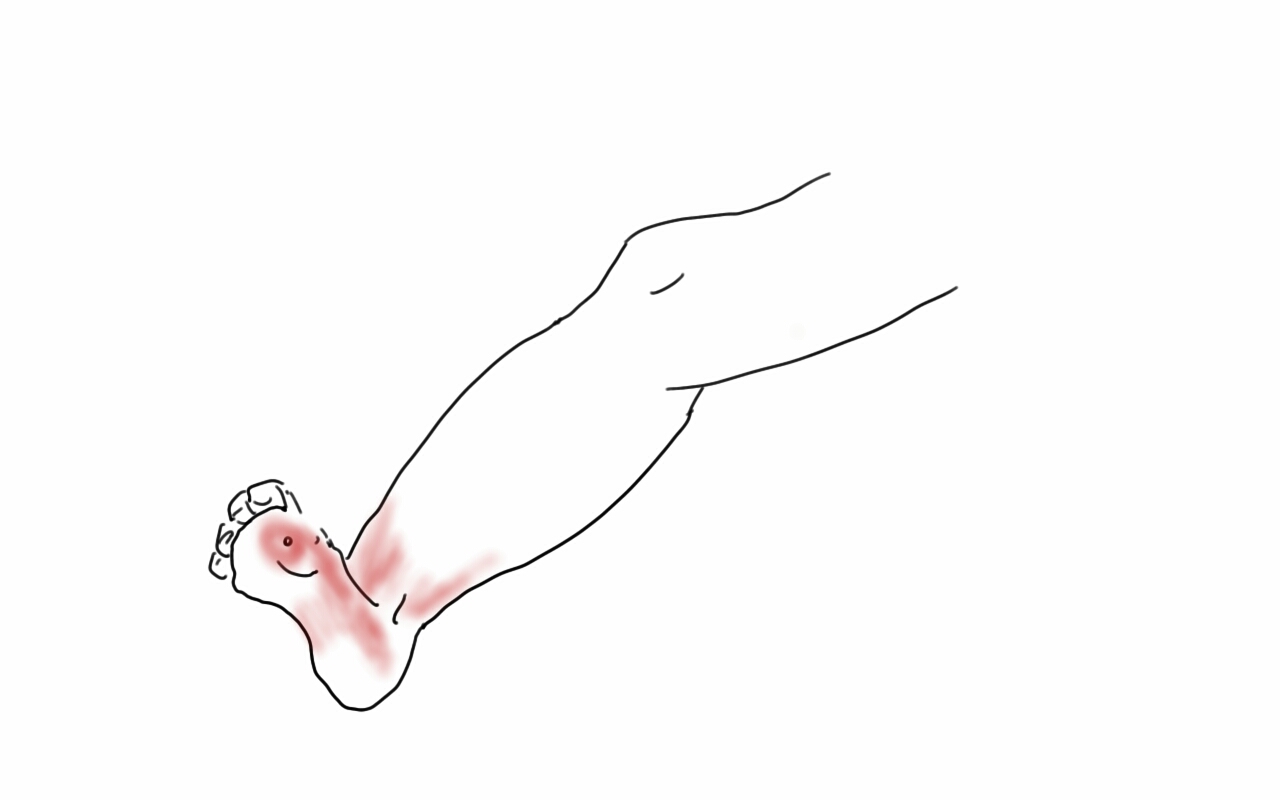
At one time, I was performing below knee amputations in the same way that most textbooks prescribe. This patient presented with severe foot and leg infection with exposed tendons and cellulitis secondary to advanced diabetic neuropathy and arteriopathy.
My sketch above showed the situation which we treated with two stage guillotine and final BKA. At the final stage, standard technique involves creating the classic flap shown below.
This is a tricky flap to make well because there are many variables -the amount of muscle left, the thickness of the subcutaneous fat, the vascular supply, etc. The biggest criticism I have of this flap is that it is prone to edema particularly in the meaty posterior flap, putting great stress on the skin sutures or staples. This then creates fat or skin necrosis in the posterior flap, or muscle necrosis resulting in wound infections and hospital readmissions, which are particularly at risk for need for further leg amputation in these patients with diabetes. I have to confess, while I could figure out how to cut the flap in the end, it was really hard to teach, and if it is hard to teach, you have to figure out a better way.
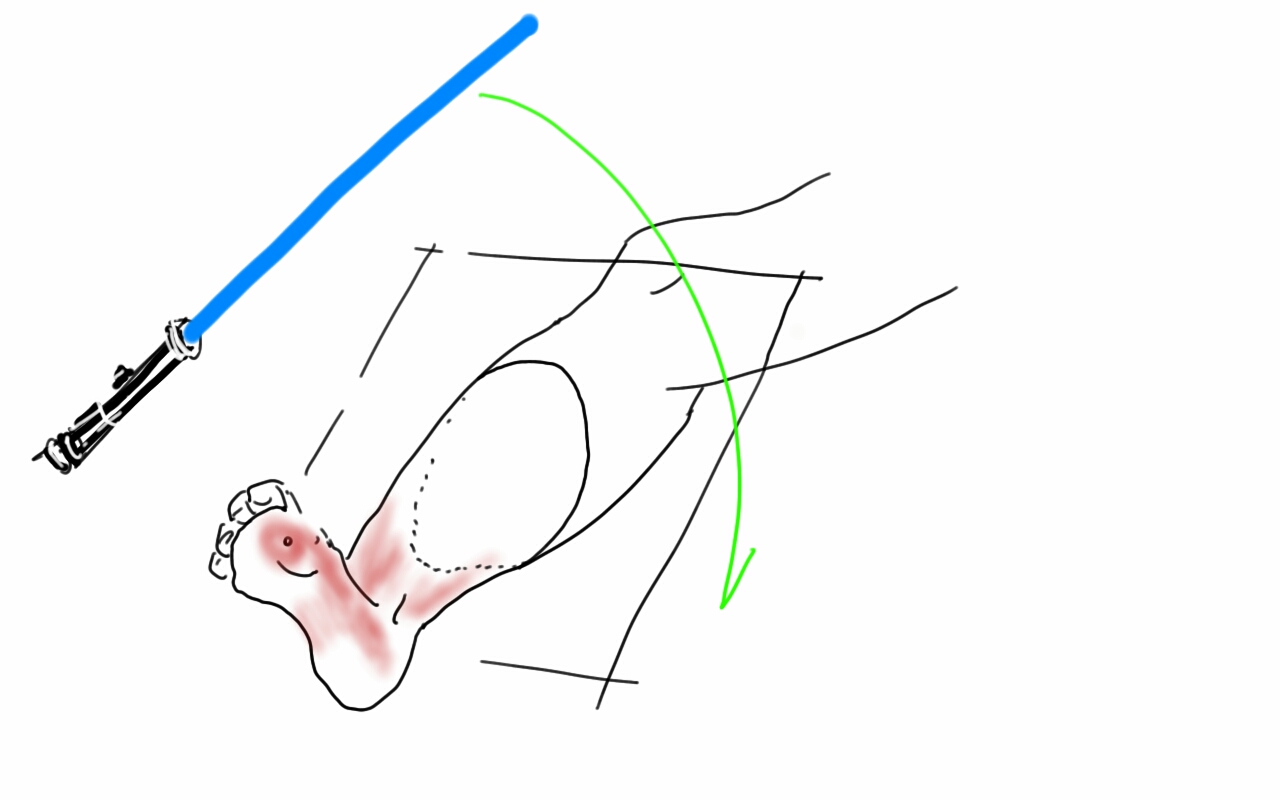
Here is the better way. The idea goes to the concept that the weight is borne in a distributive ring around the stump. The muscle on the tibia does not create a heel to bear weight on and so serves only the purpose of delivering blood to the overlying skin. So you only need the gastrocnemii and Achilles tendon for fascial closure, and maybe a little soleus. The elimination of posterior compartment muscle bulk greatly reduces the tension on the fascia and skin.
The incision can be simplified by cutting the flap along an oblique 2D plane -a light saber cut!
The posterior flap is reduced to just Achilles and a layer of soleus muscle, but otherwise, the internal bone and muscle organization is cut as below:
The skin at this point is never touched with a surgical instrument, only the subcutaneous later or fascia. Using interrupted absorbable heavy gauge monofilament (single strand of the double looped PDS used for abdominal closure is plenty of suture), interrupted buried sutures are placed in the fascia from middle outwards.
This closes the fascia and allows the skin to be closed without tension using only occasional interrupted dermal sutures and a running 3-0 or 4-0 absorbable monofilament.
The skin is dress with a single layer of Xeroform and fluff gauze and gently a compressive dressing is applied from stump to above the knee, while keeping the knee cap exposed -the knee cap is prone to skin necrosis with ACE wraps that are left unattended.
The wound’s ability to heal is now largely a function of keeping the suture line tension and edema free. Edema is the great killer of these flaps and the problem with sutures or staples here is that edema creates zones of skin necrosis under these staples that then results in a postop wound breakdown and infection. With these simple steps largely copied from our plastic surgical confreres, I have been able to create very functional stumps with low morbidity.
This patient is 3 months from her 2 stage amputation and is walking on her prosthetic leg and is very happy. Notice, the dog ears have contracted!
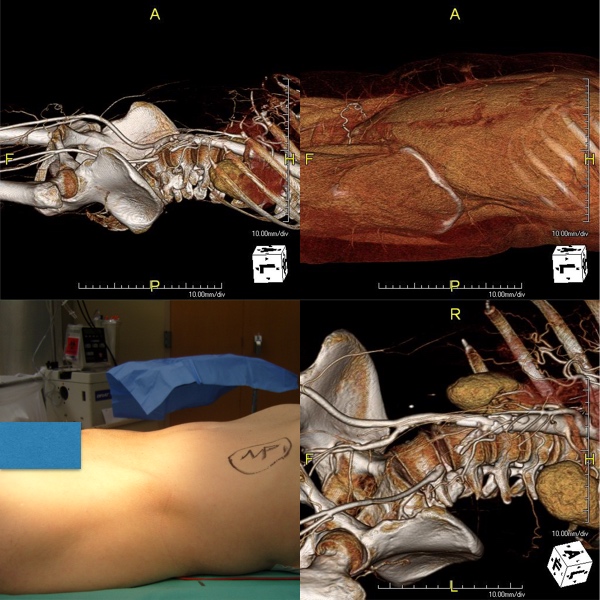
The images above show a patient with on isolated occlusion of his left common iliac artery. He was young, in his forties, but was a heavy smoker and suddenly developed claudication of his left leg which interfered with his work. He quit smoking and did not progress with exercise. Discussion involving possible stenting was made and initially offered but he turned it down because erroneously he assumed that his father’s coronary stents were the same as an iliac stent in terms of longevity. I do think that common iliac and aortoiliac occlusive disease is well treated with stents, but I felt it was possible to do a common iliac endarterectomy. We went over these images together and he settled on proceeding with endarterectomy.
The images show how well the 3D Volume Rendering, which I mentally call Virtual Reality, of CTA makes it possible to plan out operations and exposures virtually. The bottom left image shows the surgeon’s eye view of the exposed vessel.
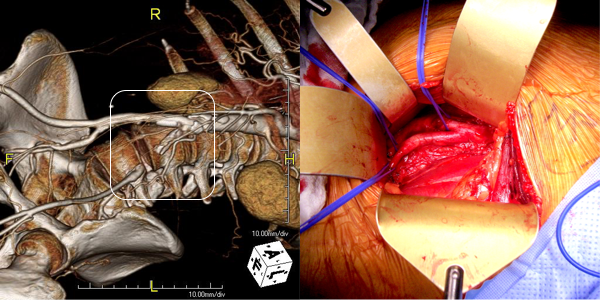
Below, the virtual and the actual are juxtaposed.
The outline on the virtual image (volume rendered) shows the areas of retraction -for the trainees, the retractor systems work to make quadrilaterals out of linear incisions, and as a rule, the incision should be twice the length of the square that you want to expose. The end points of the endarterectomy were at the aortic and iliac bifurcations.
The arteriotomy was repaired with a patch at the iliac bifurcation -the common iliac was large and was repaired primarily.
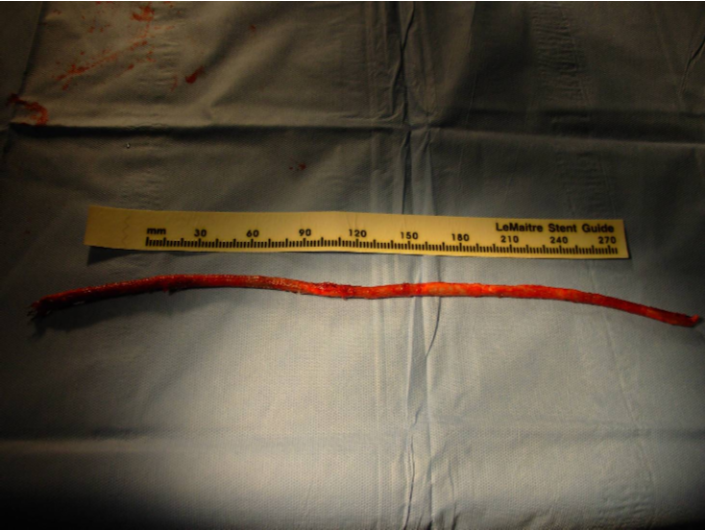
The specimen below was fibrocalcific. The thing about this disease is that the plaque truly has no endpoint -intimal thickening and mild plaque was present that could be taken all the way to the aortic root and to the feet on the other end!
This patient did very well and had palpable pulses. He did not develop neointimal hyperplasia and successfully quit smoking.
One of the exciting developments is the ongoing development of wearable virtual reality and display solutions -particularly from the gaming industry. The gaming industry ironically drives all computer imaging because that is where the money is at. The advances in imaging trickle down to medicine -the VR images seen here are the result of the same algorithms that drive first person shooting games. It would be great to see this displayed intraop on a HoloLens, on a virtually positioned screen behind the assistant!
In 2007, at which I had performed about 20 standard EndoRE (Remote Endarterectomy, LeMaitre Vascular) cases over about two years, this patient in his later 40’s presented to me with ischemic rest pain of his right foot. He was a current heavy smoker who initially had severe claudication and a TASC D occlusion of his right superficial femoral artery. Prior to being referred to me, he had undergone a mitral valve replacement from which he recovered uneventfully. He then had treatment of claudication starting with iliac stenting and a vein bypass. He had undergone a femoral artery to below knee popliteal artery bypass with reversed greater saphenous vein which became occluded after being complicated by MRSA wound infections. When this graft developed problems at the distal anastomosis, he underwent revision with a jump graft from the arm. This graft went down after he developed MRSA infection of the cephalic vein harvest site. He then underwent SFA stenting with 5 femoral stents (at that time, long stents were not available), but these occluded and his access site was the nidus of MRSA based sepsis. He had had multiple hospitalizations for MRSA infection from phlebotomy sites when he presented. He had reintervention for in-stent restenosis, first with balloons, then an extra stent, then cryoballoon therapy, each episode complicated by MRSA infection. He presented with severe claudication and nocturnal rest pain. On exam, he had dependent rubor, elevation pallor and absence of pulses, despite having fairly benign anatomy on CTA.
There was two vessel runoff below a reconstituted popliteal artery, with stent occlusion and visible stump of the vein bypass.
My options included bypass with PTFE, cadaveric vein, endovascular recanalization of the occluded stents, or EndoRE. While considering the MRSA which had been extensively worked up prior to presentation by ID including TEE and multiple cultures, it was decided that he was firmly colonized with MRSA despite efforts at eradication, and PTFE was not an option. Cadaveric vein I have used in infections with acceptable short term results -never great long term except for one individual who I inherited from a surgeon in Kansas who maintained a decade of patency of a cadaveric vein to tibial artery bypass with coumadin alone. This patient was not likely to be so lucky. Endovascular recanalization with atherectomy versus laser was considered, but I had at that point become disillusioned with those modalities in such extensive disease.
EndoRE made the most sense because it was my observation in a prior patient in whom I had unintentionally removed a 4cm stent with plaque that stents are placed inside plaques and when you remove plaque, theoretically, the stents have a layer of plaque between them at the adventitia. Also, he had none of the extensive calcium that made regular EndoRE challenging. Also, it would be repaired with native tissues through a single groin incision, and covered with a sartorius flap. And that is what I did.
The common femoral artery was exposed and the SFA controlled. The plaque dissection was started and the ring fitted around plaque and stent. There was a little more friction than expected, but I did inject via a catheter cold LR with the idea that it would shrink the nitinol a bit. Also, the wire that guided the catheter did double duty as a dissector as I was subintimal with it. The rings traveled well to the end point which I achieved with little difficulty.
Vollmer Ring Dissector around plaque & stents
The end point was dissected and required a short self expanding stent. The patient recovered well and was discharged, but as in prior admissions, developed a cellulitis on the groin wound that resolved with Vancomycin, presumably with MRSA. A CTA done at that admission showed excellent patency and he had palpable pulses.
Three years later, he underwent intervention by one of my partners in cardiology at that time for a restenosis in the mid SFA and had ballooning and a stent -the second set of stents in this patient, and by the time I left Iowa, he was still patent and walking.
This operation fails with randomly distributed TASC A lesions that develop in sites of remnant smooth muscle. I think today, I would treat with a drug eluting balloon. Thrombosis is the other failure mode, but unlike PTFE grafts, there is no thromboembolism of the outflow, rather, the SFA thromboses with reconstitution of the original state, and is amenable to thrombolysis. Smokers such as this patient and those with limited outflow are anticoagulated with warfarin.
The Europeans call this now arterial restoration. The vessel is returned to its baseline state with a full complement of collaterals which are revived. Also, compliance is restored and I believe this plays a significant role in maintenance of patency. Also, as the native tissues heal, they return to a normal ultrastructure -I have taken pathology specimen with aortic punches to perform bypasses to the other leg from external iliacs treated so, and they were microscopically and visibly normal.



































 This closes the fascia and allows the skin to be closed without tension using only occasional interrupted dermal sutures and a running 3-0 or 4-0 absorbable monofilament.
This closes the fascia and allows the skin to be closed without tension using only occasional interrupted dermal sutures and a running 3-0 or 4-0 absorbable monofilament.