


Why perform such an extensive endarterectomy when just a few stents will do? This is a valid question, given the relative safety of interventions and the durability of bypasses. There are three reasons why ilio-femoral-popliteal endarterectomy works well in my practice.
- Minimally invasive
- Restore elasticity and collaterals
- Move the inflow point from the groin to the knee
The procedure is minimally invasive. Take for example this patient whose plaque is shown above. He had a common femoral occlusion for which a common femoral endarterectomy was aborted when the prior surgeon ran into excessive bleeding. Workup for coagulopathy was negative and the patient came to me with rest pain. Pedal level pulses were not palpable, and the signals were barely there.
CTA showed that he had a CFA occlusion as well as SFA occlusion.

Because the common femoral plaque is contiguous with the external iliac plaque, it is often simpler to complete a remote endarterectomy over wire up to the external iliac origin than to try to get a satisfactory end point at the inguinal ligament -I do not like stenting across the ligament into the patch which is the usual bailout if the end point causes a stenosis. It is far simpler to apply a stent at the external iliac origin.
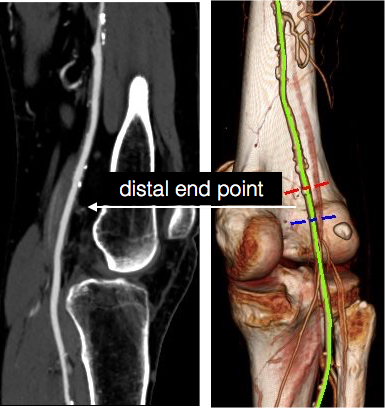
The popliteal end point was chosen where the visible plaque was no longer apparent in the patent artery. The goal is to cut across thin intima, and frequently no distal stent is required because a secure end point is achieved much like the “feathered endpoint” seen in carotid endarterectomies.

My intention was to endarterectomize the atherosclerotic plaque from the external iliac origin to popliteal artery via the groin incision marked in orange.

The video shows the setup and motion in dissecting the plaque.
The plaque came out easily (first image, top).The proximal and distal end points required stents.

The patient regained palpable dorsalis pedis and posterior tibial artery pulses. Total OR time was less than 2 hours. An ilioinguinal field block allowed for good pain control and the patient was discharged the next morning, having to heal only a 10cm wound. There is no good endovascular option for common femoral disease, and while stenting the whole SFA can be done, on more than a few occasions I have had to treat occluded “full metal jacket” SFA stents, usually by removing them. EndoRE has been shown to be superior to PTFE and almost as good as vein in the REVAS Trial when compared to fem-AK POP bypass. Going home the next day after such an extensive revascularization is not a stunt -it’s the direct result of limiting the incision and blood loss and OR time.
2. Restore Elasticity and Collaterals -Arterial Restoration
One of the components of arterial flow that is lost with atherosclerotic disease is arterial elasticity. That is the stretchiness of the artery in response to pressure. Elastic distension and recoil account for significant portions of forward flow during diastole which is lost with atherosclerotic plaque. As plaque builds up, and the artery becomes stiffer. The artery that goes through remote endarterectomy regains this elasticity. Ultrastructure from a recanalized external iliac artery sampled from a punch arteriotomy for a cross ilio-femoral bypass showed that three months after endarterectomy, the external iliac artery was ultrastructurally normal per pathology report.
Also, collaterals that were previously occluded are seen to be restored to patency. This has an important impact on patency and any future failures. The endarterectomized arteries fail due to the presence of isolated, random fragments of medial smooth muscle which cause focal TASC A restenoses. These are easily amenable to balloon angioplasty. If the revascularization fails, there is no catastrophic thromboembolism that is typical of PTFE thromboses -rather the collaterals keep segments open and it is straightforward to thrombectomize or lyse the artery and intervene as necessary.
3. Moving the inflow point from groin to the knee.
This is an important concept. One of the principles of inflow restoration is delivering large flow and pressure directly from the aortic source to the leg. Recanalizing from the external iliac to the below knee popliteal artery creates this situation below the knee, allowing for very short bypasses to be performed from the popltieal artery to tibial targets -a very useful circumstance when vein is limited. This next patient is a presented with gangrene of his fifth toe after esophagectomy for cancer, and had severe diabetes.

He had useful saphenous vein in his thigh only, some of it having been harvested in the proximal thigh for a common femoral endarterectomy. CTA showed a dilated common femoral and profunda femoral artery, severely calcified SFA and popliteal artery which were occluded, and only a patent peroneal artery as runoff.

The plan was to harvest the short segment of vein then through the same incisions, below the knee and in the mid thigh, expose the below knee popliteal artery and tibial origins, and the mid SFA. I intended to avoid the groin. The plaque was removed from the tibioperoneal trunk to the SFA origin, and the origin was stented.

This reestablished a normal inflow at the level of the below knee popliteal artery. I also did an eversion endarterectomy of the anterior tibial artery which resulted in significant back bleeding -a good sign. A short bypass was performed from the below knee popliteal artery to the peroneal artery.

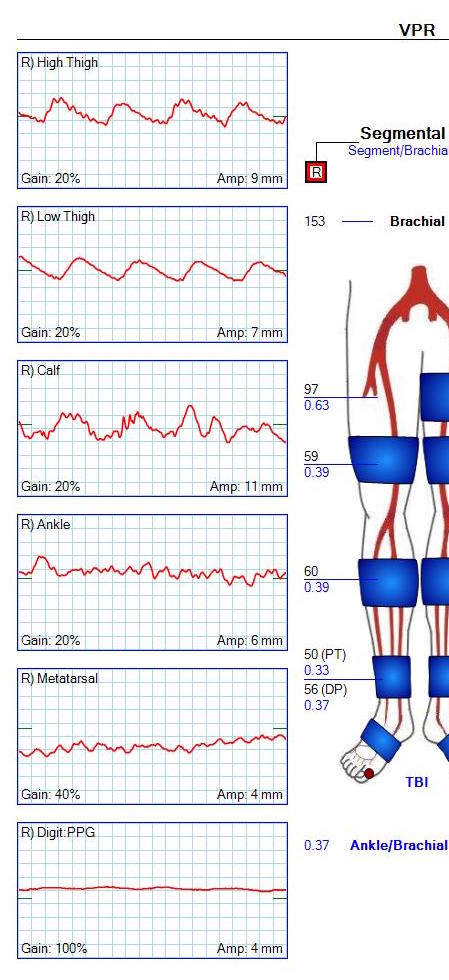
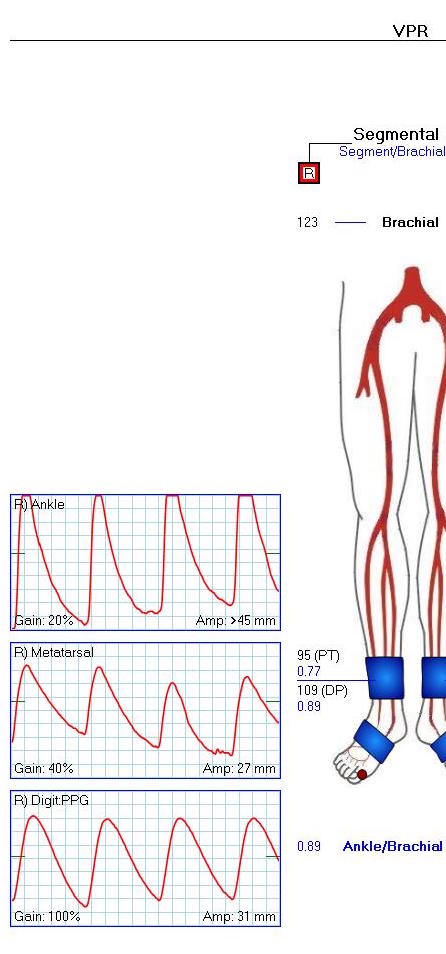
This resulted in a palpable dorsalis pedis artery pulse and excellent peroneal and posterior tibial artery signal.

The ABI improved and the waveforms predicted healing for his 5th ray amp.
This last case illustrates the point that once the conceptual inflow point is moved to the below knee popliteal artery, bypasses can become short, and durable tibial revascularizations become feasible. By avoiding a redo groin, avoiding multisegment arm vein bypass, and keeping the procedure time under 5 hours, the operation remains less invasive.
