
Median arcuate ligament syndrome has some disrepute among vascular surgeons because it does not make intrinsic sense that an isolated celiac axis stenosis, an intermittent one at that, would cause a regional mesenteric ischemia in a population that is in the literature, generally younger than the classic population seen for chronic mesenteric ischemia. And it shouldn’t, because no exceptions to the physiology and anatomy of mesenteric ischemia can be made.
The finding that some younger patients present with post prandial upper abdominal pain with associated compression of the celiac axis by the median arcuate ligament of the diaphragm dates to the 1960’s. These patients lose weight and find relief by leaning forward, standing, and crouching. They resort to small volume liquid diets in extreme cases, and more than 50 pounds of weight loss is seen.
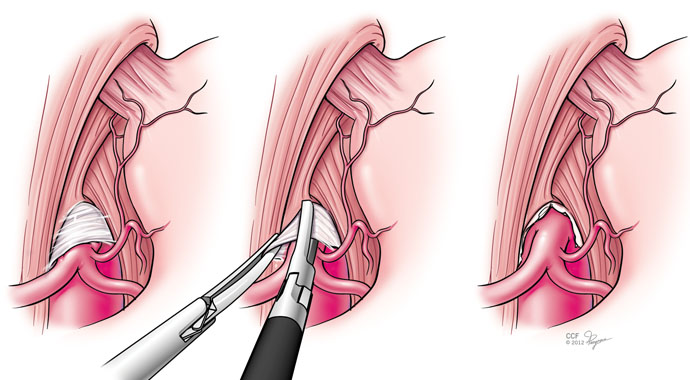
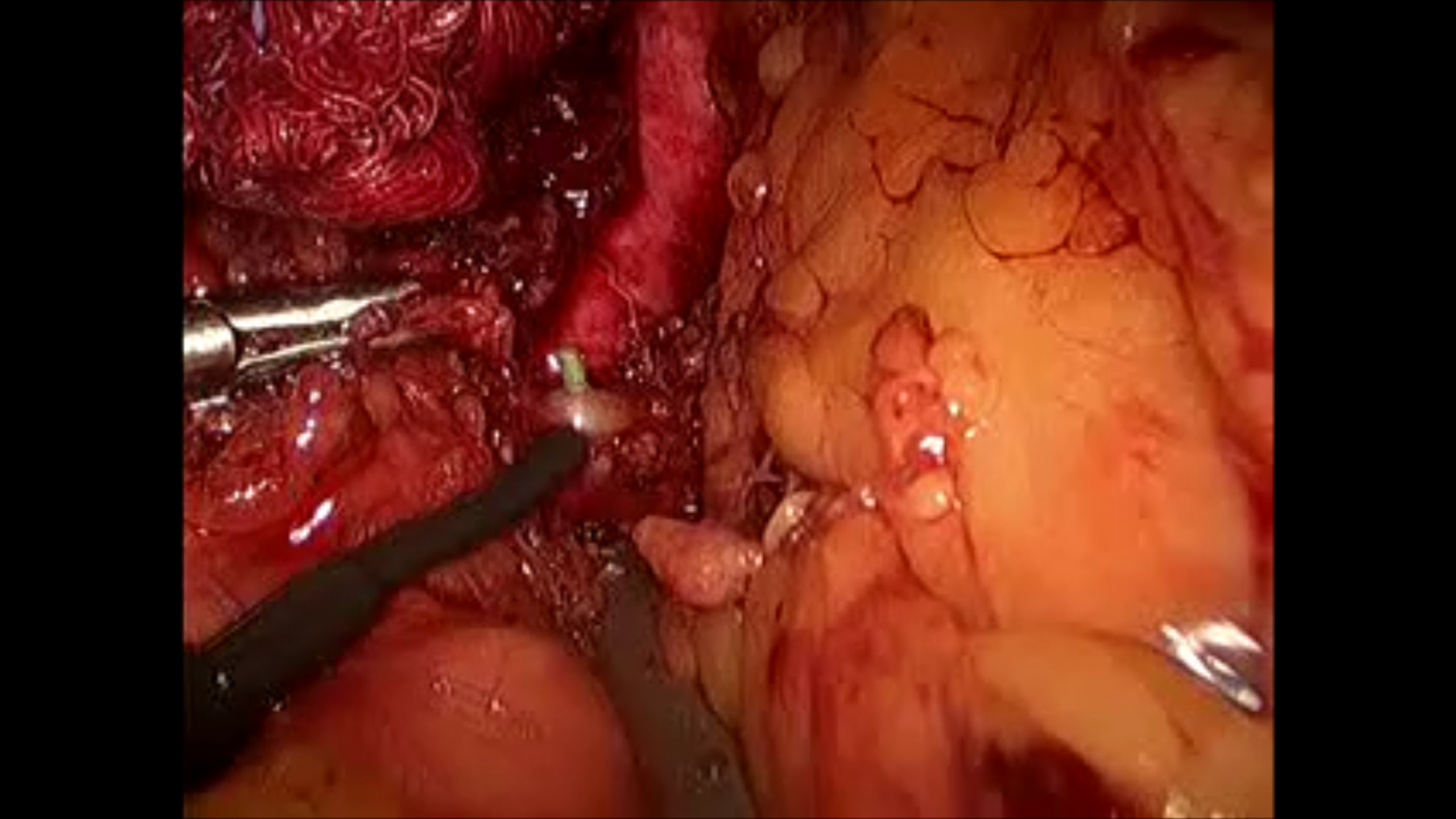
During my fellowship, we treated these with operative release of the median arcuate ligament and there would be fibrosis and the celiac plexus, nerves mediating somatic pain from the foregut, would be ablated during the dissection. Inevitably, the celiac axis would undergo a patch or bypass because of the chronic scarring on the artery due to the compression. For the past two years, in collaboration with Drs. Matthew Kroh and Kevin El-Hayek (now in CCF Abu Dhabi), these releases have been performed laparoscopically, and celiac stents are hardly ever used.
John Weber, our vascular surgery chief resident, has prepared this data and we have submitted it to the PVSS for the meeting in February. Not thinking of this as a vascular disease, but rather a nerve compression disease, much like neurogenic thoracic outlet syndrome or carpel tunnel syndrome, the pathoanatomy and clinical presentation make far more sense. There is inflammation typically and nerves are ablated, and celiac plexus block, it turns out, is an excellent screening tool when the classic presentation is not present. It is analogous to using a scalene block in neurogenic thoracic outlet syndrome. Redo operation is feasible if the original procedure fails to relieve pain completely, if the celiac plexus block works to block the pain.

One reply on “Median Arcuate Ligament Syndrome (MALS) Is Not a Vascular Disease”
Hi Dr. Park, I have the CTA and ultrasound to show MALS structure. But. My symptoms are typically different and lower abdominal, relief from leaning back not forward, not necessarily postprandrial. But we did a celiac block to rule out MALS. The block was done correctly but was 15 days ago and has made things worse. In addition to my prior pain and issues, i now have pain higher up. I’m told well the block didnt help so its not an issue due to MALS but also told the block steroid may make things worse for weeks to months. Have you heard of this? Also, i thought this may point us in another direction, but i’m left empty. and the CTA and ultrasound are still there. Can you please chat with me? i have email notifications set on so if you reply here i can then ping back somehow with my email address.
LikeLike