This podcast generated from this blog post “perfectly compulsive, perfectly smart” discusses the critical importance of not falling into the efficiency trap of algorithms and treatment pathways. Algorithmic thinking is the bane of modern medicine -ask patient where it hurts, touch the part that hurts and describe it, order labs and imaging studies, read the report and do what it says. That space between the algorithm and the truth is where AI will step in. The patient with a rare disease usually struggles within this system.
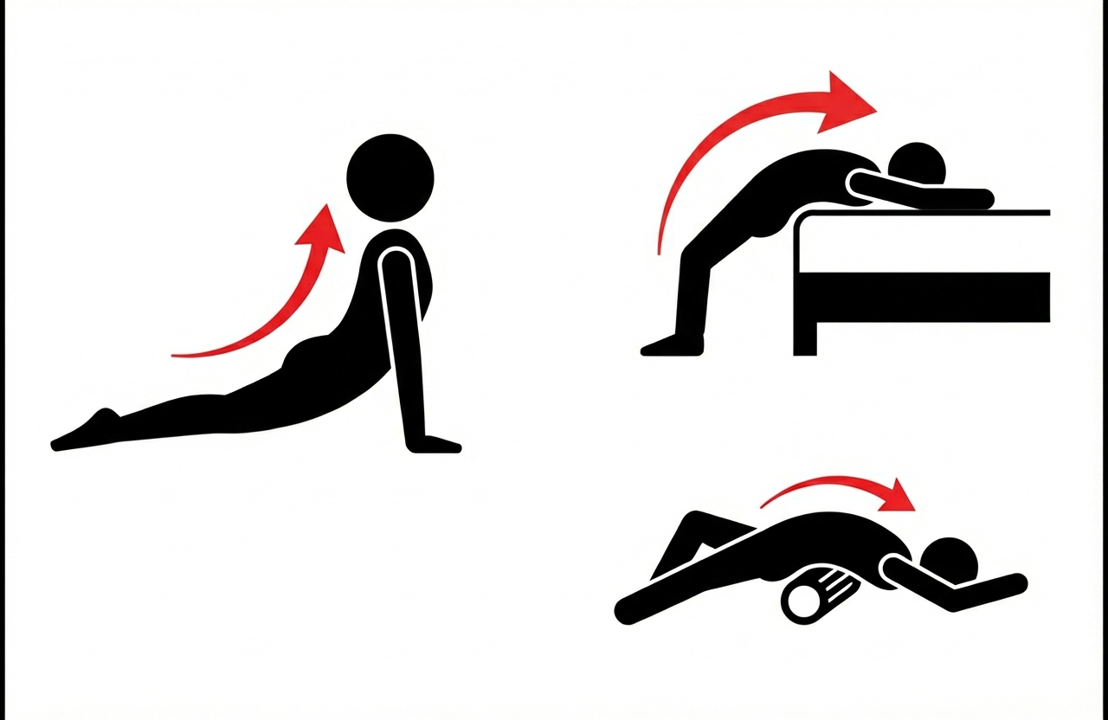
When you sprain your ankle and its on the mend, you instinctively start stretching to retain and regain range of motion, or you end up limping. The fibrosis seen in many pathology specimen of median arcuate ligaments resected surgically suggest the need to do the same -range of motion needs to be entrained with these stretches and with deep inspiration and breath holds. It should feel a bit uncomfortable.
The anecdotal evidence goes back over a decade where a patient I had performed laparoscopic MALS surgery on developed recurrent pain. He had a blockage of his celiac axis and was told to get a stent. I spoke with him in detail and given his pain with breathing and moving, I suggested starting stretches while I made inquiries about stenting where he lived (far away). He reported back after a month that these stretches relieved his pain and he no longer needed angioplasty. He is a physician and I still followup.
The other anecdote has to do with a patient I saw in Abu Dhabi who was an expat. She had classic MALS pain but her insurance would not cover surgery at CCAD and she was scheduled to return to her home country which did not have surgeons knowledgeable in MALS. I recommended stretching and eating standing up. Eating standing up relieves the pressure under the ligament and relieves any kinking of the celiac axis. She found substantial relief with these alone and left for home having regained some of her lost weight and managing her symptoms.
I recommend these stretches postoperatively to start the process of establishing a broad range of motion of the diagphragm as scarring starts on day one. The scarring is a healing process that rebuilds a median arcuate ligament much in the way that a severed Achilles tendon with regrow in a boot.
Generated from my prior posts on the biomechanical problems generated by a bipedal lifestyle, this podcast discusses those issues. This was discussed by Dr. Elen Feurriegel on her lecture series “Big Mysteries of Human Evolution” available on Audible where she describes the human spine as a stack of teacups and saucers supporting a bowling ball.
The patient information paper on median arcuate ligament syndrome has had a surprising amount of traction. I had Google’s notebook LM create a podcast.
Last December, I received an email from a LOCUMS company begging for Christmas coverage at a nearby hospital. It offered an eye watering $330/hr for coverage during Christmas week and weekend. A friend posted about this on X, and it was edifying because no vascular surgeon gets this as regular pay, but it reveals the current market price of an on-call vascular surgeon, at least as much as travel nursing, and the willingness of hospitals to pay for it, reveals the true value of an experienced nurse. If you wonder why it takes so long to see a specialist in 2026, the answer is in the fact that very few people were biting for this offer to be cast so far and wide.
The fact is that no hospital can do things with sharp objects without running into the need for a vascular surgeon.
References
Ojeda LM, Arcila SM, Nunes VA, Duarte CM, Papi M, Jacobs DL, Malgor EA, Malgor RD. The value of vascular surgeons in modern health care systems: A systematic review and meta-analysis. J Vasc Surg. 2025 Oct 28:S0741-5214(25)01865-8. doi: 10.1016/j.jvs.2025.07.062. Epub ahead of print. PMID: 41167378.
Kim Y, Weissler EH, Williams ZF, Mohan S, Coleman DM. Defining the Value of Vascular Surgery Service at a Tertiary Academic Medical Center. Ann Vasc Surg. 2024 Dec;109:198-205. doi: 10.1016/j.avsg.2024.06.040. Epub 2024 Jul 24. PMID: 39059626.
Powell R, Brown K, Davies M, Hart J, Hsu J, Johnson B, Makaroun M, Schanzer A, Shutze W, Weaver F, White J; SVS Valuation Work Group. The value of the modern vascular surgeon to the health care system: A report from the Society for Vascular Surgery Valuation Work Group. J Vasc Surg. 2021 Feb;73(2):359-371.e3. doi: 10.1016/j.jvs.2020.05.056. Epub 2020 Jun 23. PMID: 32585182.
Johnson CE, Manzur MF, Wilson TA, Brown Wadé N, Weaver FA. The financial value of vascular surgeons as operative consultants to other surgical specialties. J Vasc Surg. 2019 Apr;69(4):1314-1321. doi: 10.1016/j.jvs.2018.07.035. Epub 2018 Oct 24. PMID: 30528406; PMCID: PMC8386947.
This article went up earlier this year and it was an oversight to not post it here on my blog. It is an article explaining MALS for the lay public drawn from my clinical experience going back ten years. Our approach is still a work in progress as each patient is comes with a unique presentation. Here is the link
Today, I got up at 630, made some coffee, and Zoomed in on our morning report at our main campus hospital. I have a patient there who I will be operating on tomorrow and wanted to know the current status of the patient. Once the report was over, I brushed my teeth and drove into my hospital which is a regional community hospital. I had an angiogram for a patient who was having a problem with blood flow to the leg. The cath lab was ready to go at 0800, and I was done by 0900, where I quickly ran over to to my office for clinic. My fellow who was doing her community rotation helped me with the angiogram, and then came over to clinic where I saw 27 patients from 0900 to 1600hrs, two of them virtually. At 1600hrs, I had a hospital committee meeting where I am the chief of surgery for my community hospital, and at 1700, was done. I ate a snack as I finished up some paperwork, and got on another Zoom meeting of my institute with over a hundred people to have an update meeting. I then drive to my golf club, and got on the range and hit golf balls for 30 minutes, then got on the putting green and practiced for another 30 minutes. Then I drove home and had dinner with my family. I watched highlights of a football (American) game I recorded over the weekend, while reading email, then sat down to write this before I showered and went to bed.
This week I have 9 cases scheduled -several angiograms and interventions, a leg bypass, a few fistula creations, and a laparoscopic procedure (I’m one of the few vascular surgeons who do laparoscopic surgery). As I sit in bed, I listen to a journal article read to me by the voice of Gwyneth Paltrow (it’s AI) -I find it easier than actually reading the thing, and then I watch a few TikToks, read Reddit, and then go to sleep around 2300h. Cycle starts again in the morning, but will wake at 0530 to get to the main campus hospital to perform an operation. Arriving at main campus on a Wednesday, we have a combined grand rounds with the whole Surgery Department prior to operating.
Lifestyle On weekends, when I am not on call, I still catch up on my patients from a report from my trainees or my nurse practitioner who makes rounds. I even do this sometimes when I’m out of town. Usually, I play competitive golf with members at my club -the more pressure the better. I find competition to be relaxing. Afterwords, I come home and write, read a little, and watch sports depending on the season or golf. My writing is sometimes work-related, sometimes in my journal. I kept a personal blog for over ten years on golfism.org. I am working on a novel -have been for a decade but not making much progress. I read mostly nonfiction but will listen to audiobooks of science fiction -currently marching through all the Dune prequels written by Brian Herbert, the son of Frank Herbert, the author of Dune and its original sequels. I am working on a grand unifying theory of circulation.
Procedures As a vascular surgeon, I perform operations in the traditional open fashion, and endovascular procedures which are a done with imaging from x-ray. Occasionally, I do laparoscopic surgery. The open surgical procedures include operations on the aorta and its branches, and on arteries in the legs, arms, and neck. I also work on veins throughout the body. The patient arrives with a set of conditions, a prior history, and an examination, and given a problem, you evaluate it with various tests which can be blood tests, vascular tests, imaging studies like X-ray, Ultrasound, Vascular Lab Studies, CT scans and MRI’s. This is called the workup -getting data to plan a procedure. Knowledge of anatomy and physiology and biomechanics of flow are crucial to put together a plan that will be successful in treating the disease with low complication rate and good durability. The procedures require a great deal of planning and often I include my colleagues within my department and those in other specialties to get their insights for making a plan that accounts for the reason for operation, plan for operation, contingency plans, and recovery in the hospital, and healing outside the hospital. You can see some of these cases on my blog, vascsurg.me.
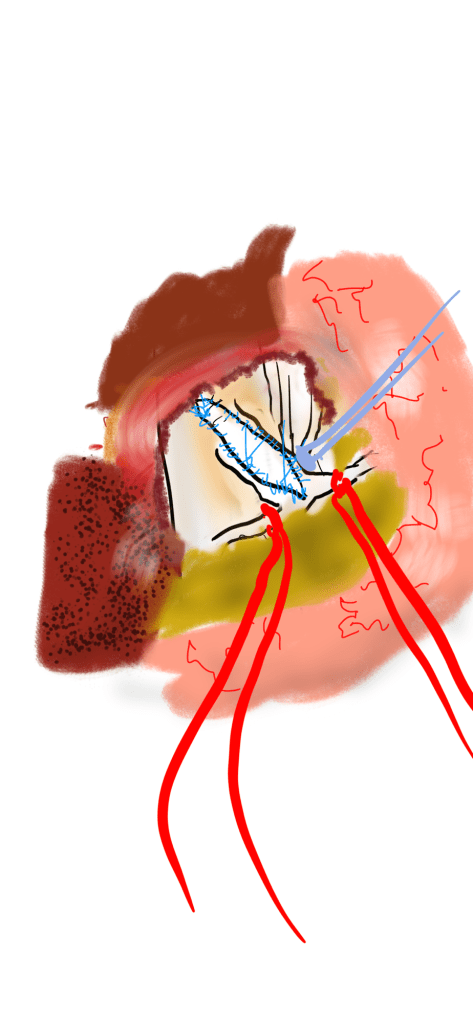
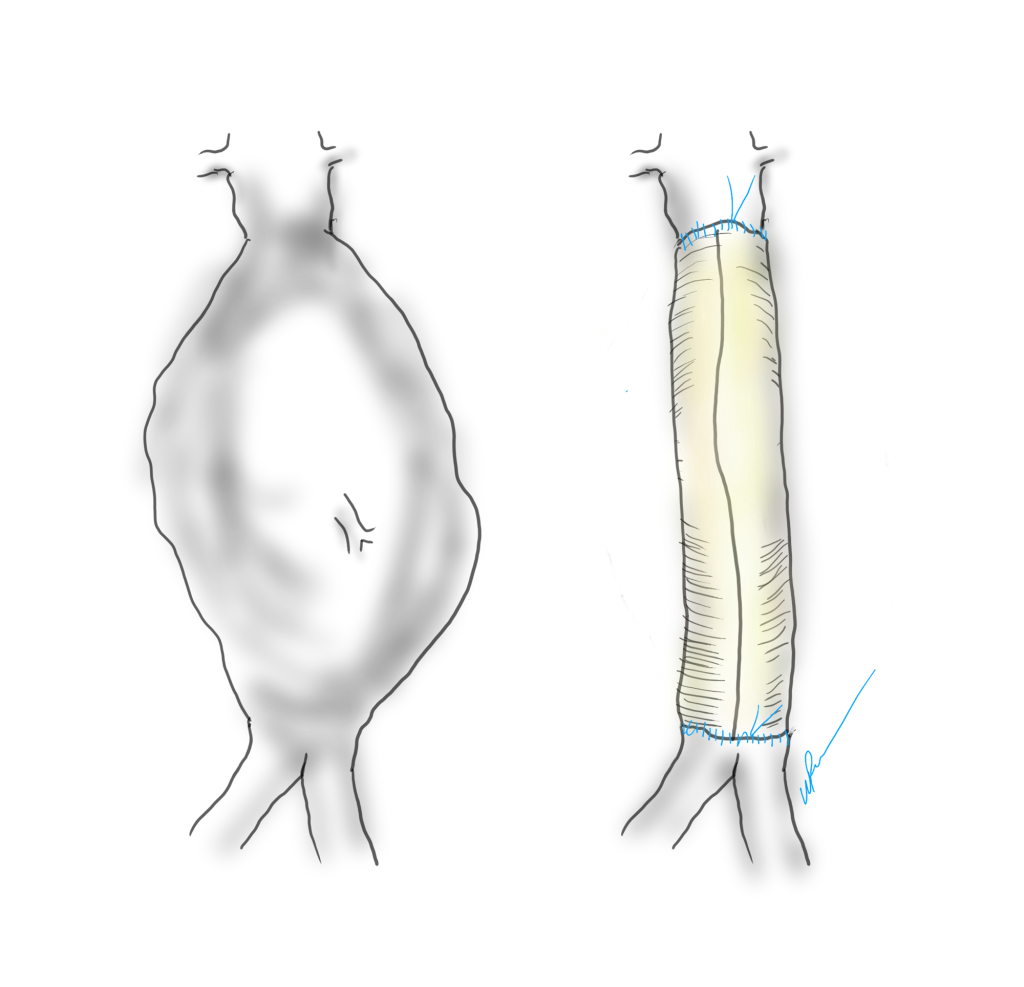
The image above shows a common femoral artery aneurysm presenting as a pulsatile mass in the right groin. The first image on left is an arteriogram (a sketch of one) that I would get prior to surgery. The patient is also suffering from pain in the right leg due to a lack of blood flow because his superficial femoral artery (SFA) is occluded and his profunda femoral artery (PFA) is open but has a blockage at its origin where the aneurysm ends. I plan the surgery and execute it. During surgery, things may pop up -good things like finding an otherwise pristine SFA filled with plaque. Removing the plaque, it becomes a great conduit for replacing the aneurysm and avoids using an expensive graft which can become infected -your own tissues fight off infection better than graft.
In the F1 Movie, Brad Pitt’s character describes a sense of pure driving, being in the flow, being completely at peace on the road. The best moments in surgery, I reach a flow state where actions follow one after the other. It’s a form of spiritual ecstasy, to be completely focused and present. Even better is having the patient do well -to be able to walk without pain and the fear of possibly losing a leg or dying.
Who should not do vascular surgery. By definition, anyone not trained in vascular surgery. Successful vascular surgeons come in all shapes and sizes, but they share common traits -grit, focus, some intelligence, and hand-eye coordination. That would mean those who give up easily, have trouble with focus, are unintelligent, and have poor dexterity should not go into vascular surgery. The saddest cases are when the desire to be something does not match up with the reality. It is possible for non-vascular surgeonsto make a living doing a focused practice around varicose veins for example, but a good vascular surgeon is hard to create. Also, you should not do this for money or prestige, there are easier ways to get money or prestige.
Who should go into vascular surgery. Anyone who thinks they might like it should certainly look into it. The best way is to directly observe a vascular surgeon at work. That is the whole purpose of the rotations in medical school. Sadly, many medical schools do not offer much time in a surgery rotation and vascular surgery exposure is inconsistent. Our society has been working hard for over a decade to improve this and we are seeing it in the excellent applicants to our training programs. The best candidates are driven people with a track record of academic excellence, but the qualities that make a good surgeon are harder to define. Desire alone is insufficient and sadly academic excellence, while it will get you into the door, doesn’t predict who will be a great surgeon. There has to be grit -an ability to persist despite hardship. There has to be a nimble mind that can solve problems quickly. And there has to be the physical hand skills that define surgery but somehow have been dropped from the initial evaluation of candidates for surgery.
Who should not go into surgery. Based on my answers above, those quick to give up, are unintelligent, and poorly coordinated should not go into surgery. I would add to this lazy, dishonest, and sociopathic. No criminals please.
There is no perfect answer to this. I knew a fellow who did not score well on tests and was rejected from medical school five years in a row, but eventually got in and completed a residency in a surgical subspecialty and has a very successful practice. While he was being rejected from medical school, he spent five years in the lab, and he could do open heart surgery on dogs very well, was coauthor on numerous papers, and his surgical skill was excellent -like if you were stuck taking tennis lessons from a professional for five years but never playing an actual game. There are also many examples of people who were told too late that they were no good for surgery.
What you should not do is listen to just a single person who has a poor opinion of you. You should examine the situation and decide if there is some truth to the issue, but you need at least three opinions. For example, I would like to be a professional golfer. I can get at least three people to tell me honestly that this is a bad idea. I would like to be a writer. I can get at least three people to tell me honestly this is a good idea. You get the picture. In medical school you will rotate and work with many people and you will have grades and feedback. You need to get honest opinions as you move forward. You need to study hard and get great grades because no matter what you do, your patients will be depending on you.
In George Orwell’s Animal Farm, under the dictatorship of the alpha pig, Napoleon, the pigs who represented the nomenklatura of the farm chant the slogan “four legs good, two legs better,” after initially declaring “four legs good, two legs bad” during their revolution. They clearly understood the luxury afforded by a bipedal lifestyle, because in rising on two legs, you get arms and hands which can do many things like caress a baby or wield a cudgel. What the pigs in the parable weren’t realizing were the consequences of a bipedal lifestyle.
When Lucy, the Australopithecine, bipedal hominid ran about on two legs, she did have the use of two arms and hands. Possibly an adaptation to living in tall grasslands with few trees, the ability to stand tall like meerkats, allowed the biped to see far into the horizon for big cats who probably loved the big brained hominid for the high calorie meal inside the hard skull -many fossils from this time show puncture marks from the incisors of medium to large cats.
The walking and running put heat stress on the brain, and the tool use which happened incredibly early and is observed in the chimpanzee, likely drove the selection for a larger brain (more neurons will allow for one to lose some neurons to heat stress but stay in the game), but it created likely the first problem for our ancestors -discharging a cantaloupe sized head through a pelvis that was small to begin with but now also reshaped for bipedalism. We still suffer from a childbirth process that no other mammal faces -birthing a less than fully cooked baby -a tradeoff for that giant head.
Standing also meant the load bearing was shifted 90 degrees with long term consequences. For our ancestors who only lived about 20-40 years if the chimps are correct, this wasn’t a big deal as arthritis and tendinitis didn’t preclude eating and breeding and didn’t affect them until they were old. But with modern sanitation and social structures, we are reaching 100 years and the majority of the problems of the integument -the bones and ligament, the low back pain, the sore knees, the ratchety hips, can all be explained by our bipedal lifestyle. Your arm is 30-50 pounds of meat and bone and supported only by muscles off your spine, and your blood vessels and nerves traverse a narrow passage through these muscles and your first rib. Your diaphragm with 5-10 pounds of heart, lungs, and blood sits on first branch artery off of your aorta. Your veins, designed to drain blood from your organs, have to do so with over a meter of static water pressure and your sump pumps only work when you are walking. Muscles and their tendons are stretched tight in the odd way that upright walking and running demands, compressing blood vessels and nerves. All of this weight is put on your feet which have to deal with up to a ton of pressure with running…
I’ve talked about this concept many times before but never had a chance to put it together like this talk. I may write an article. Looking back, I did this blog post (Link).
I am grateful to Ms. Mei Nortley and Mr. John Raphael for the invitation to give this talk.
Recently, an AI was fed the world literature on AAA repair and asked about guidelines and superiority of open versus endo repair. It concluded that the past twenty year, endografting has only benefitted the physicians and the device companies (this was present at VEITH). I recommend open to patients likely to benefit from it. I recommend EVAR same way. They are not equivalent especially when patients end up getting insurance denials. I hope it isn’t too late to turn this boat around and train surgeons on open techniques that seem to have been abandoned in many parts of the world.
I will touch on vascular compression disorders like median arcuate ligament syndrome, thoracic outlet syndrome, nutcracker syndrome, pelvic congestion syndrome, popliteal entrapment syndrome, varicose vein disease. Presentation given to the Oxford University vascular unit. Will be streamed on Oxford Vascular Collaterals.
Topic: “Vascular Compression Syndromes: The Consequences of a Bipedal Lifestyle” – Dr Woosup Michael Park, MD
Time: Sep 13, 2024 12:45 PM London, 0700 Central Daylight Time