
Our journal club today is discussing one of the many trials that have tried to validate endovascular renal denervation to control severe hypertension. One of the devices I was on trial for back in the 00’s was the CVRx Rheos trial which stimulated the carotid sinus using a surgically placed electrode and generator. While the approval trial failed in the US, it was approved in Europe and my observation of over 30 patients who had this at my center at that time was that it was effective. So effective that I believe many patients stopped taking their pills in exchange for electrical energy -some patients required at least once a year generator changes, often more, but they had normal blood pressures and less to none of the side effects of their medications which frequently exceeded 5 agents.
I have observed that on the carotid baroreceptor, which is shaped like an aneurysm by the way, there are paired vasovasorum in the pattern seen above. The only other time I have seen paired arteries is with a nerve. The baroreceptor nerves are very hard to see, but they are there and you can find them between these paired vessels.
The observation that the baroreceptor looks like an aortic aneurysm isn’t a silly one. The area of maximal wall tension is in regions of greatest curvature change and these, teleologically, would be the shape of a baroreceptor. The stiffening of these regions with atherosclerotic plaque would decrease the signal sent to modulate blood pressure and heart rate, and create a pathologic cycle of increasing pressures in response to increased vessel stiffness and vice versa. Just saying.
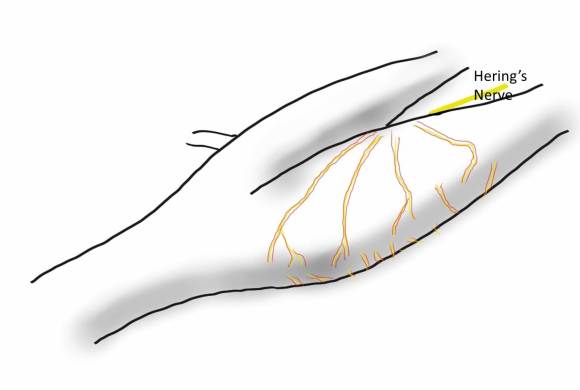
I began to wonder if restoring the elasticicty of these vessels and the shape of the baroreceptor would have a lasting impact on blood pressure. The operation is eversion carotid endarterectomy with sparing of Hering’s nerve.

The plaque can be removed without stripping the carotid sinus nerves, resulting in restoration of the sinus/baroreceptor complex.

This would result in bradycardia/hypotension, which I have observed in a percentage of my eversion endarterectomy patients. Cutting the nerves results in hypertension, and was the subject of a paper from Montefiore (reference).
However, the proximal ICA at the carotid bifurcation was mobilized circumferentially to facilitate its transection from the CCA at the carotid bulb. During this approach, carotid sinus nerve fibers derived from the glossopharyngeal nerve and innervating the carotid body within the adventitia of the proximal ICA were routinely divided (Mehta et al.)
In that paper, hypertension was seen in 24% of patients undergoing eversion CEA with denervation compared to 6% undergoing standard endarterectomy, and as an aggregate occured for a prolonged period of time:

The hypotension and bradycardia that I observe in nerve sparing eversion endarterectomy appears to be transient, but it is my unstudied observation that some of these patients subsequently have a lower need for blood pressure medication. This will deserve further study, but may explain the variable results of denervation procedures aiming to control hypertension. To some extent, all blood vessels are innervated and provide an aggregate signal to the CNS. Without understanding the central pathways of hypertension, the baroreceptors offer the best way of controlling blood pressure without medication like lighting a flame under a thermostat to get the building colder.
Reference
J Vasc Surg 2001;34:839-45.
