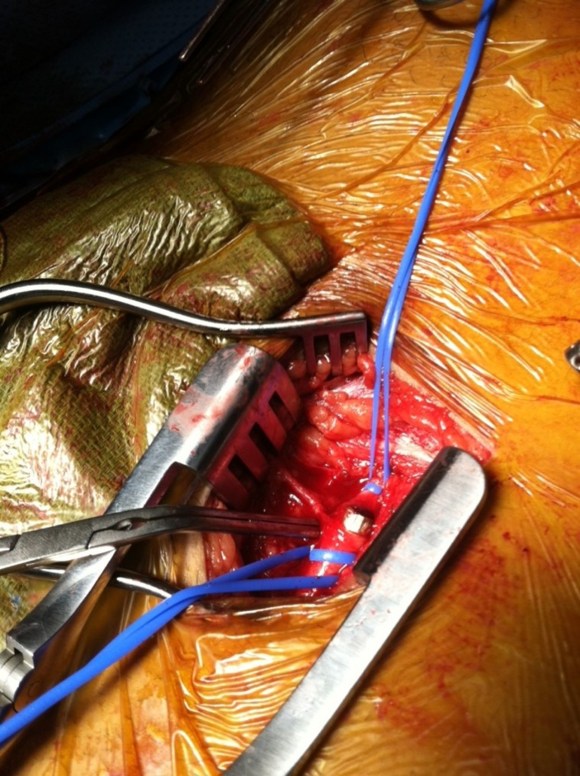
While I was a site investigator for the CVRx Rheos Trial, a device that induced hypotension and bradycardia by stimulating the carotid baroreceptor with electrical energy to control resistant hypertension, I noticed that Hering’s nerve can be readily identified by accompanying arteries which show up as paired red lines. The baroreceptor complex is a pressure transducer and the maximum dP/dt can be transduced in areas of maximum curvature change. If you recall those tension maps of aneurysm rupture points, they occur in areas of maximum curvature and inflection points -wouldn’t a baroreceptor be constructed to sense pressure and change in pressure here? Hering’s nerve comes out over these areas. It struck me that most of the patients with carotid disease are hypertensive and it may be a disease cycle that occurs with stiffening of the baroreceptor, decreased parasympathetic tone, and hypertension as the output signal with subsequent vessel injury and plaque formation and worsening stiffness -a non virtuous cycle.
The nerve probably wraps around the origin of the internal carotid artery or wherever the curvature is best suited for pressure transduction. If you visualize the bulbous origin of the ICA as the belly of the guppy, the arteriotomy is made traditionally on the side facing you which is on the side and across at least half of Hering’s nerve -on the lateral surface of the guppy. If you make instead an arteriotomy on the belly of the guppy, and preserve as much of these nerves as possible, it would be theoretically possible to reconstitute a baroreceptor, maybe the dominant one (there is a sidedness to the baroreceptor strength).
There is an intriguing consequence to cutting the nerves -for example in skeletonizing the ICA for an eversion. Eversion endarterectomy done this way is associated with greater incidence of postop hypertension than standard endarterectomy (ref 1,2). The question is if the converse -if reconstituting the baroreceptor can bring decreased need for anti hypertensive medications or even hypotension and bradycardia -is true and if there is potential for applying this as therapy for hypertension as well as stroke risk reduction.
References
1. J Vasc Surg. 2012 Aug;56(2):324-33.
2. J Vasc Surg. 2001 Nov;34(5):839-45.