

The patient was shot in the right shoulder and had walked to the emergency room with some dyspnea and back pain. CXR showed a right sided pneumothorax but no bullet. The paper clip on the 3D VR view of the CTA shown above is the entry wound. The green line traces the centerline of the aorta, aortic arch, and the right carotid system. The patient’s assailant was shooting from a balcony of a movie theater. Vascular surgery was consulted for loss of pulse in left leg during trauma workup.
CT scan of the chest and abdomen showed blood in the mediastinum and haze around the distal thoracic aorta.

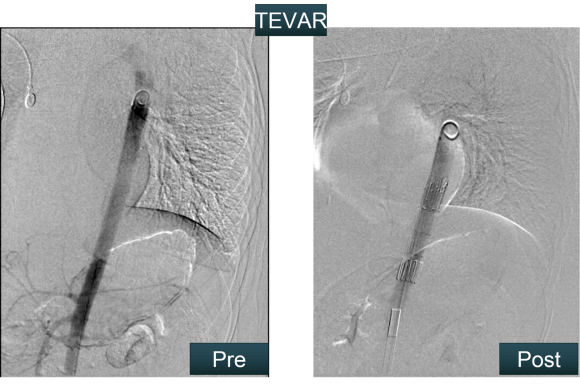
Remarkably the patient remained stable. My plan was to cover the aortic perforation with a stent graft, but an appropriately sized graft for patient’s size was not available at that time in 2009, so we used a Zenith RENU cuff. The patient on examination had an absent left femoral pulse. I chose to explore this and use it as the access site of the TEVAR. I also made sure the detectives put on scrubs to receive the bullet as US laws about evidence requires witnessed removal and acceptance of criminal evidence.
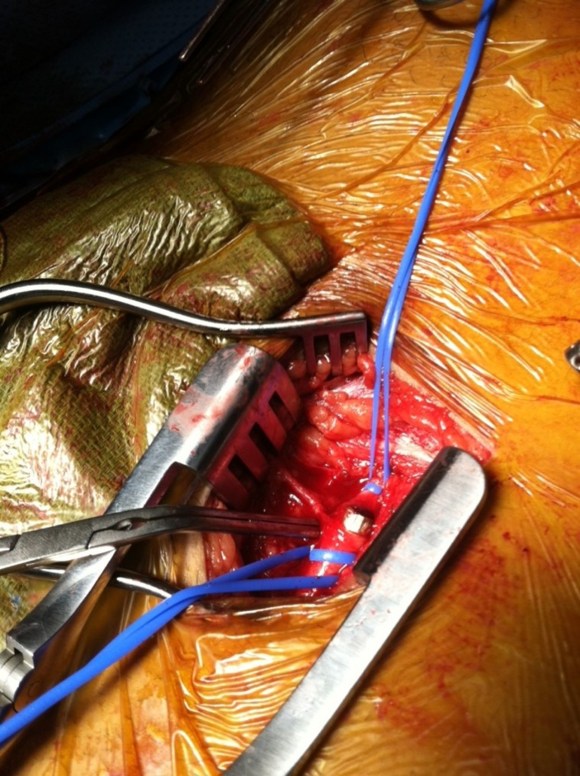
The cutdown revealed the bullet (9mm round) to be lodged in the common femoral artery. It was placed in a kidney basin with a loud clank and handed off to the peace officer for processing.
The bullet managed to miss the esophagus, heart, major pulmonary vessels, upper abdominal organs, and gently nestled in the aorta and embolized to the femoral artery in the emergency room.
The RENU cuff’s delivery system was long enough –at the time of this procedure, smaller diameter thoracic stent grafts were not available and in the setting of trauma with younger patients, particularly female patients, this was a problem. An aortic cutdown was sometimes necessary to deliver a 24mm aortic cuff up near a tear due to deceleration at the ligamentum arteriosum of the pulmonary artery and aorta. The patient recovered well and this case report was written up by Dr. Jared Kray who is now a vascular surgery fellow in Missouri –the article is in print for the January issue of American Surgeon.
