

The patient presented with complaint of right leg swelling and pain that became unbearable as the day progressed. He had had a prior bout of septic ankle joint which occurred after treatment of infected hardware in the other ankle. He did have an aspiration of his joint but no major surgery. His local specialist performed arteriography, found an arteriovenous fistula, and referred him after concluding that an endovascular repair was not possible.
On examination, he had dilated leg veins and a boggy, tender leg without chronic venous stasis changes. There was an audible bruit over the ankle where the fistula was identified. It would have been near the puncture site of an aspiration needle. CT scan showed the arteriovenous fistula along with chronic changes on the arterial and venous sides due to the increased flows.

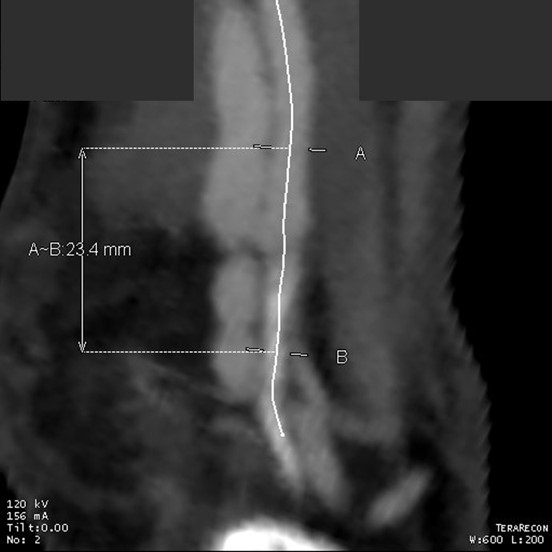
This included relative dilatation of the anterior tibial artery and the outflow veins. One of the animal models of iliac aneurysm involves creating an arteriovenous fistula of the femoral artery at the groin of a rat –this was an arduous operation done under a microscope which was the final exam of a microsurgery course during my fellowship, but I digress. Arteries respond to perturbations of flow by dilatation, elongation (engendering tortuosity), and plaque formation. Two areas of naturally occurring elongation are the internal carotid artery and the external iliac artery –in both cases, it is sometimes necessary to straighten and cut out excess artery. A high number of patients with tortuous internal carotid arteries –those with kinks and loops, have aortic aneursms. In the case of the external iliac artery, this has been used in the past as conduit for infections of the common femoral artery.
He had the clinical triad for an arteriovenous fistula that persists and grows –trauma, inflammation, and good venous outflow. The pain was due to venous hypertension but I suspect some regional compartmental steal and pressure may be at play as well, but that’s hard to prove. It makes me think there may be a way to create AV fistulae for dialysis access using these principles.
The 3DVR imaging was very helpful in planning the operation, particularly the incision and exposure.

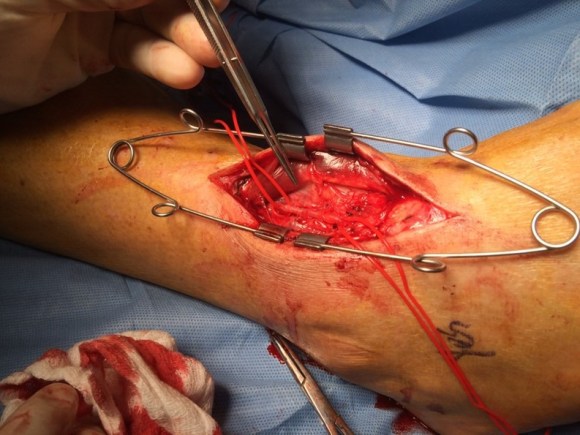
Is there an endovascular option? Probably, but why? What are the costs of coils and glues when a few clips and sutures will do? This patient did very well with ligation and division of the fistula. The real magic is our imaging and image processing capabilities.
