A great New Yorker article relays the efforts scientific efforts focused on Ebola and the calculus of ZMapp allocation.
Author: docpark
golfist

Link to Science article re genomics of current outbreak
I keep a small notebook around with me to jot phone numbers, clinical data, and random ideas. It is a kind of fossil of the pre-digital age that persists. When someone finds my box of these notebooks, they will think my life was consumed by frustrated novel writing, grocery lists of esoteric food items, and vascular ailments. They would be correct. Here are my top ten thoughts about Ebola.
- Ebola is an RNA virus which likely has its origins in the most ancient recesses of life on earth. Likely during the prebiotic Hadean era, roughly a quarter billion years after earth solidified and liquid water started to coalesce into oceans, these molecules began replicating themselves within the primordial soup that made the whole planet a single cell, with chemical reaction times stretched over eons rather than seconds. When some of the molecules found shelter in enclosing the sea in a phospholipid bilayer, maybe some sudsy foam at the edge of an acid sea, these replicating molecules followed. The ribosome, transcription RNA, and other ribonucleotide based molecules in our cells are the friendly remnants of these molecules. Ebola is the stranger that comes to take life from our cells.

- This RNA world hypothesis is an idea first posited in the 80’s by Dr. Walter Gilbert, and RNA prefers an acidic, anaerobic environment, which is what is proffered once Ebola takes hold in the vasculature. The liver seems to be the place where Ebola’s fire ignites, and it offers the low oxygen, acidic environment that echoes the flavor of that primordial soup.
- Edema due to vascular leak results in eventual dehydration, and more anaerobic, acidic environs to run in. Patients who are well hydrated and kept euvolemic seem to do better per reports on the web. To this, I would add well oxygenated which would become harder to achieve with third spacing into the lung. Is there a role for active alkalinization. Patient’s who have filled their lungs with fluid -is there a way to push forward development of an oxygenator that is inserted into the central veins.
- Coherent light can cause particles of specific dimensions to resonate. Can this be a way of disrupting 80nm width virus particles? A light emitting catheter that uses laser energy to split virus particles while leaving other blood elements intact -for advance infections. Plasmonic resonance I believe it’s called.
- The current movement of Ebola patients out of general hospitals puts into sharp relief the importance of training and will in controlling difficult medical problems and the role of specialty centers of excellence. Medecins Sans Frontieres are able to achieve in a rude tent in the fever jungle what country club hospitals cannot. Generations of domination over infectious diseases has bred complacency as few remember polio quarantines and no one remembers the Spanish Flu pandemic of 1918. At Columbia P&S, in the student lounge, there was a plaque dedicated to the 20 medical students who died while caring for victims of that pandemic that took millions of lives. At that time 20 years ago, dying from an infectious disease seemed quaint and atavistic, just bad luck like dying from a plane crash or shark attack. Now, we’re not so sure.
- n=e^(qt) where q determines the rate of exponential growth. What is different about this outbreak compared to numerous others? The q may be different because of different factors but it starts with knowing the sequence of this Ebola compared to others. Also, the population density or temperature or inoculation may have been higher because of deforestation, climate change. Time will tell. The evidence thus far is that it is not airborne.
- The thing not often talked about in the Irish Potato Famine is the poor potato. Crowded into unending fields of monoculture, often by cloning via sprouting the “eyes” of the potato, it left it vulnerable to the potato blight. We are an unending field of monocultured humans when we look at cities of 10, 20, 30 million pressed back to front. Typically, human overpopulation is seen to be treatable through some combination of education, development, and draconian laws, because it is in our nature to be fruitful and multiply. Even plagues and wars fail to remove our reproductive drive. I feel least optimistic about this, and feel fraternity with the Irish Potato.
- Soap and water. Alkalinizing and oxidizing. Bleach. Peroxide. Alcohol? How do you kill something that is lifeless? We will be dealing with this for a long time but it won’t be like HIV. I have been stuck with needles from HIV+ patients and lived, and my biggest immediate fear then, even 10 years ago, was hepatitis, not HIV. This different.
- Hackathons solve some hefty problems related to data security. We don’t have hackathons for these kind of medical and scientific problems. All the scientific disciplines have specialized to the point that its rare for people of different disciplines to synthesize and collaborate. I have socialize regularly with a physicist and live across the street from virologists. I had half a mind to bring them all together, and my physicist friend had the same thought. He works on plasmonic resonance -I won’t get into the math but at the size of nanoparticles, which are the size of Ebola virions, things resonate when hit with a particular frequency of light resulting in chemical changes. The problem is its too dangerous to work with Ebola directly, but the principles of phototherapy for example could be worked out in a model using plant RNA viruses -and we have a world leading lab here in Cleveland. Every university town in fact has the human capital to do something, but the way we have structured science and discovery works against multidisciplinary work. There should be a Cleveland Project, a Boston Project, a Berkeley Project, an Austin Project and so on. Let the hackathons begin.
- We survive as communities. The biggest lesson Zombie movies have for us is that the real monster is the unfriendly human. The other hidden lesson is that going it alone is unwise. We are evolved as social animals that hunt in packs and keep secure in numbers. That means we need each other more than ever before.

The usual situation is a multiple redo or infected groin with heavy scarring. Woody is the proper adjective. The common femoral artery may be obliterated or buried in the scar but a small profunda or its major branch may be accessible. Or you just run into it and get bleeding. Rather than bemoan your fate, you may be able to make a purse out of sow’s ear by exposing the artery and sliding in an appropriately sized Argyll shunt. Backbleeding into the shunt means that you haven’t dissected (hopefully) the artery, and now you have control over the surface edge of an artery. You can then clamp the shunt. You can assess your situation and decide that spending another two hours digging out two centimeters of 3mm artery may not be worthwhile, but you also decide that it is important to preserve this vessel.
It is straightforward to anastomose graft to the arterial stump. The shunt keeps you from narrowing the anastomosis, as you are well aware from carotid shunting. While you are doing this, if you have a Rummel tourniquet or vessel loop around the distal external iliac, you can feed the leg via this shunt as long as you remember to have the graft over the shunt. And remove it when you are done.
Another scenario is in revascularizing an intercostal, lumbar artery, or backbleeding posterior origin accessor renal but don’t want to do it right away.


- What are the indications for surgery?
- What kind of operation are you planning with what approach?
- If different (open, endovascular, or hybrid) approach is preferred by you, please briefly elaborate. If not, explain why?
- What are the anticipated risks, recovery, and followup?
I started having my trainees (yes, you) email me answers to these questions for an upcoming case and it has been working pretty well. This starts a conversation. This exercise gives the trainee time to think about their plan, do some reading, ask questions, and anticipate outcomes so that an unexpected one would be rare. It also gives me a record of a meaningful interaction so that later assessments don’t devolve into flash judgment, gut feeling, first impressions, or recall of latest misdemeanors.
Not infrequently, I have trainees whose opinions differ from mine, but they base their arguments on solid evidence and clinical findings specific to the patient and not just the general topic. They express a nuanced understanding of that particular case and bring in fresh perspectives from their diverse backgrounds and education. I think to myself how honored I am to have such hard working, brilliant minds to teach; I make sure to tell them how absolutely wrong they are.
Categories
All Those IVC Filters
Thousands of filters were placed over the past decade and the cows are coming home to roost. My feeling is that if a removable filter goes in, there must be an appointment or mechanisms in place to arrange for it to come out, anticoagulation must be started as soon as feasible, and kept on as long as possible if the filter is to remain in. Failure is infrequent for the conical designs, and not an issue if the filter is removed. How long after implant that a filter can be removed seems to be a moving target. In my personal experience, I have safely removed them out to two years, but I have partners who have gone beyond that by multiples. Two rare late failure modes of IVC filters can be devastating and life threatening.
IVC Perforation

This patient developed a vague upper abdominal pain and plain radiography showed the filter on a tilt. CT shows the legs of this Simon Nitinol filter extending into the right kidney and duodenum.

The 3 D VR images assisted in operative planning –as is my habit, it rotate the image into the surgeons-eye perspective to plan the incision.


The green arrows point to the exposed legs of the filter once the right colon and duodenum were rotated out of the way. The duodenum required only a serosal suture. The vena cava above and below the filter and both renal veins had to be controlled to remove the filter which was extirpated in pieces. I have had to do this about once a year or two. The youngest patient I operated on was a 20 year old who had a filter placed after a car accident at 17, but never had it removed. The legs of the filter had eroded into his duodenum causing an abscess.

Iliocaval Thrombosis
The figure below shows two panels with a Trapease filter associated with an iliocaval thrombosis. This patient had cardiovascular collapse and severe bilateral lower extremity edema after a long car ride.
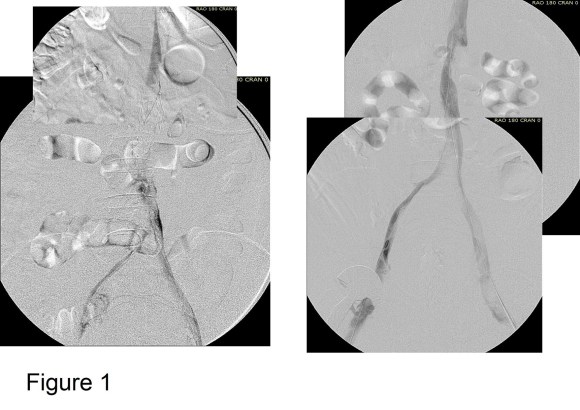
Venography showed iliocaval thrombosis. Thrombolysis was started and the second panel on right of Figure 1 shows the result.
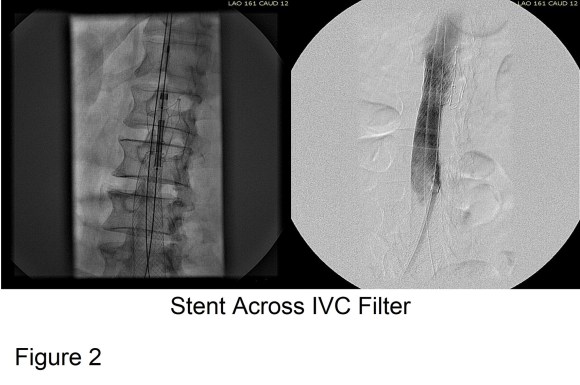
Large WallStents were used to support the recanalized iliocaval system from the common femoral veins to the filter. A Palmaz stent was deployed across the filter (Figure 2).

Figure 3 shows the final result. Interestingly, stents placed across the inguinal ligament into the common femoral vein seem to do fine in contrast to those placed in the artery. IVUS is necessary to confirm good results. Acceptable short term, and durable mid to long term results are reported.
Remove Them While You Can
Filters should be considered a short term therapy to decrease the risk of pulmonary embolism, and should be removed as soon as it is safe. There seems to be no magic time interval beyond which removal cannot be attempted. If permanent filter placement is planned, it should only be for established indications.
Categories
October Journal Club
October Journal Club (October 21, 2014) is approaching. The papers chosen by the presenters are linked below. Please refer to the club format and rules, also attached.
Presenters/Papers:
D. Hardy – Endovascular Repair of Type B Aortic Dissection
H. El Arousy – EVAR v Open
D. Virvilis – evarsurveillance3years
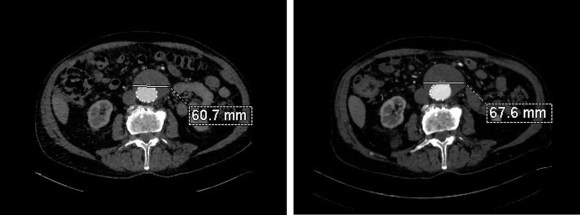
The patient had undergone an uneventful EVAR, but in followup had developed AAA sac growth. Pictured above are the post deployment CT’s from 1 month and 6 months. Reviewing the original aortogram, you can see that there was flow into the sac very late via an iliolumbar collateral.

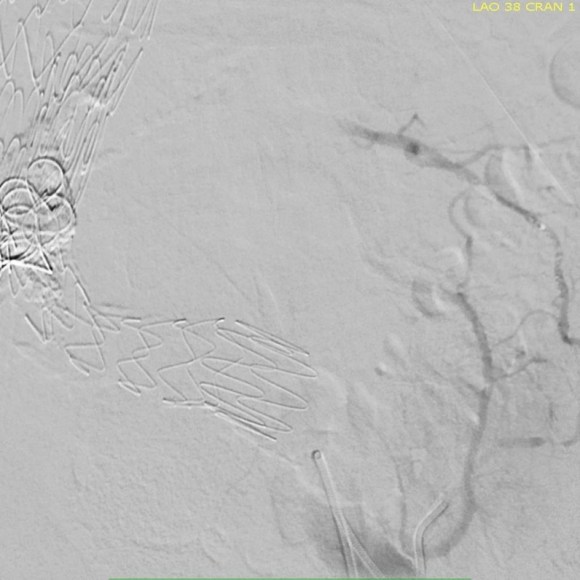
Plan was made for arteriography and intervention. As discussed in an earlier post, 3D VR was very helpful in planning access to the type II endoleak, particularly in plotting C-arm angles and access vessels.


The 3D-VR image view on Aquarius Intuition (TeraRecon) predicts a camera angle of 50 degree LAO to see the branch leaking to the lumbar vessel causing the leak.
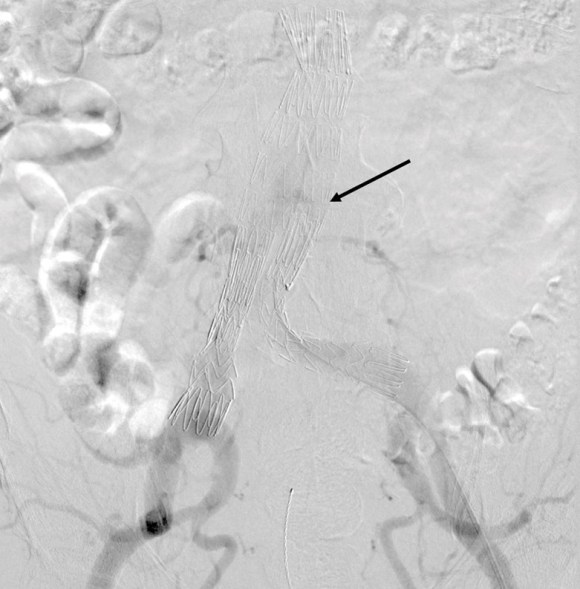
Initial aortography confirms the absence of a type I or III leak in early phase.

Later in the phase, the endoleak can be well seen, corresponding to the CTA.
I do an intraoperative transabdominal duplex of the aorta. I have submitted this technique for presentation and eventual publication, but briefly, using an abdominal probe on the abdomen, the sac and endoleak can be readily visualized, and the source of the leak confirmed.

The inferior mesenteric artery which is so often involved is not in this case, and can be easily seen with duplex in patients who are NPO and under general anesthesia. I perform these studies myself, as they are far less challenging than when a patient is awake.
Selection of the branch vessel is straightforward as the CTA well illustrates the course of the source iliolumbar vessel. The CTA even showed the loop that was challenging to traverse. The sequence of access involved IIA, branch access with a glide catheter, placing a Rosen wire for anchorage, and pushing the sheath over the glide catheter into the branch vessel, giving stability. Further access into and across the loop was then possible with superselective catheters based on an 0.18 wire system.


Once access into the AAA sac was achieved, coil embolization of the leak cavity chased by glue (NBCA) allowed for obliteration of the endoleak.
Duplex ultrasound confirmed effective closure, with absence of perigraft flow.

Using duplex in this fashion adds another dimension to the treatment imaging and has the potential for reducing radiation dose and contrast volume.
The patient in followup has shown sac shrinkage. The other treatment options are: direct lumbar puncture, open surgery with sac marsupialization and oversewing of leaks, and laparoscopic ligation of lumbar arteries. I have tried all of these, but this went as easy as could be expected and I credit the ability to visualize the entry path in 3 dimensional virtual reality. The toughest part was negotiating the loop, but a shaped 0.18 glide wire simplified this.
In 2006, Sheehan et al [J Vasc Surg 2006;43:657-61] reviewed an 7 year experience from 5 academic centers. 1909 patients had EVAR with various endografts, and there was an overall 15% rate of type II endoleak. Most resolved within the first year. No significant variation by endograft design appeared to correlate with type II endoleak, which makes sense, although TALENT graft had the highest rate. Spontaneous resolution was common. Late endoleaks were frequent. No conversions were due to type II endoleak. Higashiura, Greenberg et al [J Vasc Interv Radiol 2007;18:975-981] reviewed the CCF experience with the Zenith graft and type II leaks. Of 204 patients with suitable followup, there was a 17% rate of early type II endoleak. Of these, only a 7 of 18 patients with persistent leak developed sac enlargement. Most type II endoleaks spontaneously resolved in followup. No variables could predict persistence of type II endoleak. Treatment prevented sac enlargement.
Silverberg, Marin et al [J Vasc Surg 2006;44:453-59] found similar rates of type II endoleaks -16%, in a study group of 965. Spontaneous resolution occurred in 36% in a mean time of 14.5 months. Treatment was reserved for sac enlargement. 8.4% of those with type II endoleaks experienced sac enlargement greater than 5mm. The vast majority of patients had a benign course. Regression analysis revealed cancer, CAD, COPD were associated with earlier spontaneous closure of type II endoleaks.
Ruptures can occur with persistent type II endoleak [Jones, Cambria et al. J Vasc Surg 2007;46:1-8]. Selective treatment of those with persistent leak and sac growth >5mm seems to be a safe and cost effective approach [Steinmetz, Sicard et al. J Vasc Surg 2004;39:306-13].
Link to type II endoleak papers
 Completion angiography fits into the range of things that many of us were taught to do because it might help avoid the problem of early graft failure. I remember a time in the nineties when vascular surgery was synonymous with terrifyingly long bypass operations that sometimes worked. Back in that preinternet era, all day bypass operations were capped at the end with a flat plate arteriogram. As with all things archaic and historic, I firmly believe that our trainees should feel comfortable with this type of on-table arteriography because not every place will have a corridor of rooms with robotic c-arms. I feel that each trainee should feel comfortable wheeling in a portable c-arm, assembling it, turning it on, put in patient information, and perform a study. But I digress. The completion arteriogram clearly has a role in bypass surgery, but I question its usage as a “I do it all the time” routine. When anything is written in stone, it immediately takes on a hallowed, sanctified aura, usually taken on during M&M’s when the person at the podium intones beatifically looking skyward, “the completion arteriogram showed no abnormalities.” Science is about questioning the status quo and backing up practice with evidence.
Completion angiography fits into the range of things that many of us were taught to do because it might help avoid the problem of early graft failure. I remember a time in the nineties when vascular surgery was synonymous with terrifyingly long bypass operations that sometimes worked. Back in that preinternet era, all day bypass operations were capped at the end with a flat plate arteriogram. As with all things archaic and historic, I firmly believe that our trainees should feel comfortable with this type of on-table arteriography because not every place will have a corridor of rooms with robotic c-arms. I feel that each trainee should feel comfortable wheeling in a portable c-arm, assembling it, turning it on, put in patient information, and perform a study. But I digress. The completion arteriogram clearly has a role in bypass surgery, but I question its usage as a “I do it all the time” routine. When anything is written in stone, it immediately takes on a hallowed, sanctified aura, usually taken on during M&M’s when the person at the podium intones beatifically looking skyward, “the completion arteriogram showed no abnormalities.” Science is about questioning the status quo and backing up practice with evidence.
The purpose of the arteriogram is to evaluate the anatomy for treatable lesions. Screening for these lesions can be just as easily performed with handheld pulse Doppler and if needed, duplex ultrasound. In my experience, the triad of pink toes, palpable pedal pulses, and multiphasic signals in the distal anastomosis is more than enough evidence to start drying up and closing. In this particular case shown in the picture above, the anastomosis looked pristine, but the signals were weak and monophasic in the distal anastomosis despite palpable pulses. Arteriography reveals the reason below, but frankly, the arteriogram was dispensible even in this case (trainees –reason why?). In fact, arteriography takes care of the surgeon more than it does the patient. Tan et al [J Vasc Surg 2014;60:678-85] for the Vascular Study Group of New England, including my friend Dr. Alik Farber, reviewed the VSGNE database and found that a strategy of compulsive completion studies which included angiography or duplex ultrasonography, did not improve short term or 1 year graft patency.

I have used many different flavors of image post processing software including Osiris, Vitrea, and now Aquarius, aka TeraRecon. But I notice that outside of endovascular planning, people rarely use the virtual 3D reconstructed images (the pretty pictures) for anything other than posting images for publication in JVS, and even there I think we have reached saturation.
I have found 3D reconstruction to be especially useful for open surgical planning, and that is by doing two things. First, on viewing the 3DVR data, I reorient and center on the surgeon’s perspective, using left button to rotate the picture around the zero at the center of the screen, and the right mouse button to grab the whole image and recenter as necessary.

I then window-level in tissue density -this is done by pressing both the right and left mouse buttons, but you can choose this off the menu.

I can plan the incisions and exposures from any angle -in this case, I can see the saphenous vein and its relative proximity to the CFA to perform an in site bypass to the AK POP. And I see the loci of the tributaries that I may need to ligate.

This is a powerful tool that is often overlooked.
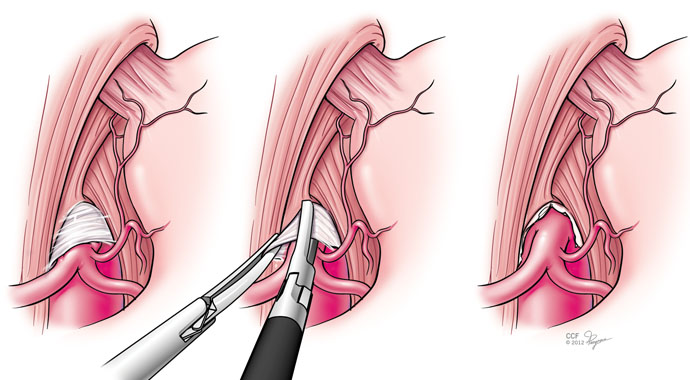
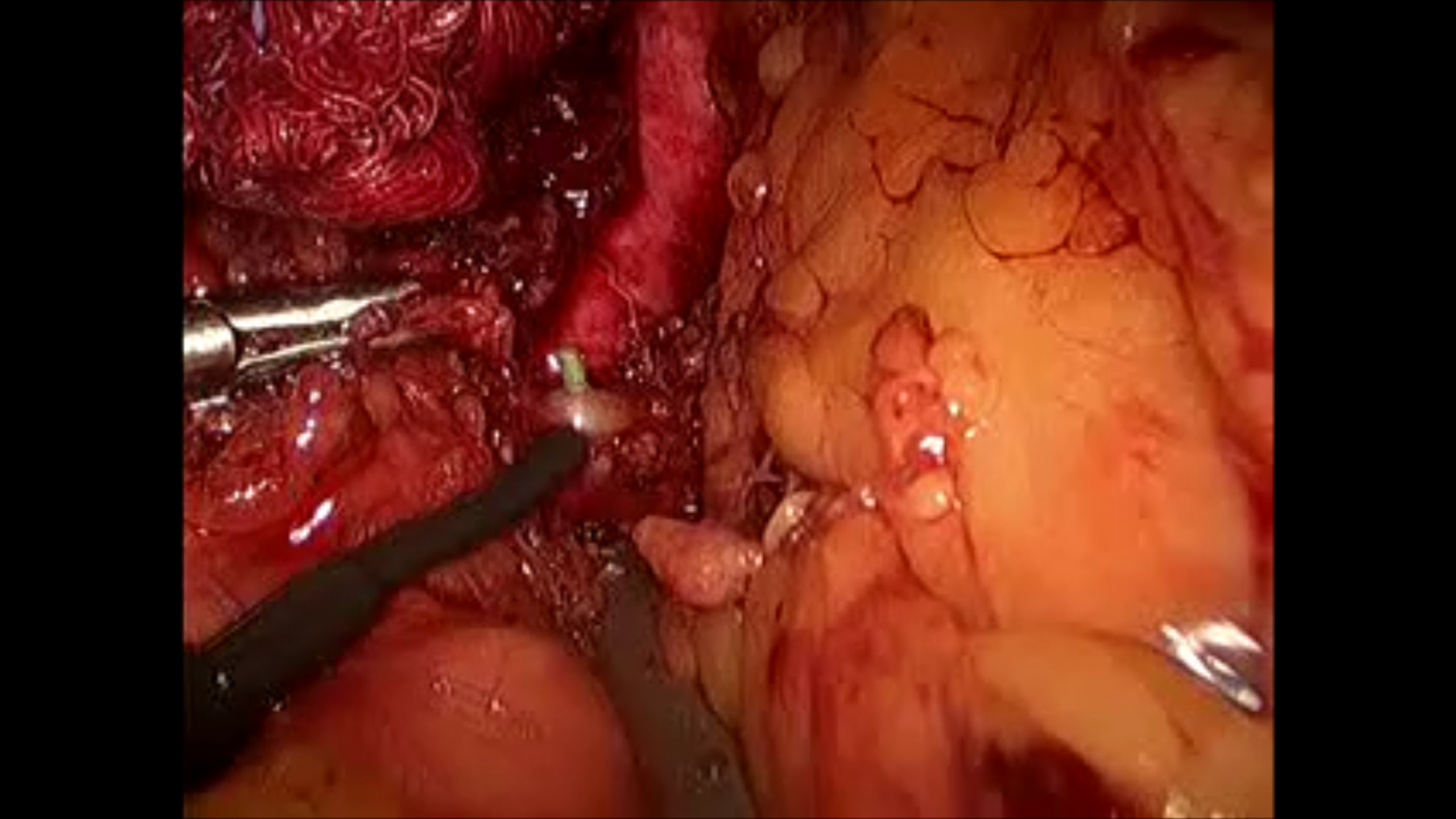
Median arcuate ligament syndrome has some disrepute among vascular surgeons because it does not make intrinsic sense that an isolated celiac axis stenosis, an intermittent one at that, would cause a regional mesenteric ischemia in a population that is in the literature, generally younger than the classic population seen for chronic mesenteric ischemia. And it shouldn’t, because no exceptions to the physiology and anatomy of mesenteric ischemia can be made.
The finding that some younger patients present with post prandial upper abdominal pain with associated compression of the celiac axis by the median arcuate ligament of the diaphragm dates to the 1960’s. These patients lose weight and find relief by leaning forward, standing, and crouching. They resort to small volume liquid diets in extreme cases, and more than 50 pounds of weight loss is seen.
During my fellowship, we treated these with operative release of the median arcuate ligament and there would be fibrosis and the celiac plexus, nerves mediating somatic pain from the foregut, would be ablated during the dissection. Inevitably, the celiac axis would undergo a patch or bypass because of the chronic scarring on the artery due to the compression. For the past two years, in collaboration with Drs. Matthew Kroh and Kevin El-Hayek (now in CCF Abu Dhabi), these releases have been performed laparoscopically, and celiac stents are hardly ever used.
John Weber, our vascular surgery chief resident, has prepared this data and we have submitted it to the PVSS for the meeting in February. Not thinking of this as a vascular disease, but rather a nerve compression disease, much like neurogenic thoracic outlet syndrome or carpel tunnel syndrome, the pathoanatomy and clinical presentation make far more sense. There is inflammation typically and nerves are ablated, and celiac plexus block, it turns out, is an excellent screening tool when the classic presentation is not present. It is analogous to using a scalene block in neurogenic thoracic outlet syndrome. Redo operation is feasible if the original procedure fails to relieve pain completely, if the celiac plexus block works to block the pain.