
Thousands of filters were placed over the past decade and the cows are coming home to roost. My feeling is that if a removable filter goes in, there must be an appointment or mechanisms in place to arrange for it to come out, anticoagulation must be started as soon as feasible, and kept on as long as possible if the filter is to remain in. Failure is infrequent for the conical designs, and not an issue if the filter is removed. How long after implant that a filter can be removed seems to be a moving target. In my personal experience, I have safely removed them out to two years, but I have partners who have gone beyond that by multiples. Two rare late failure modes of IVC filters can be devastating and life threatening.
IVC Perforation

This patient developed a vague upper abdominal pain and plain radiography showed the filter on a tilt. CT shows the legs of this Simon Nitinol filter extending into the right kidney and duodenum.

The 3 D VR images assisted in operative planning –as is my habit, it rotate the image into the surgeons-eye perspective to plan the incision.


The green arrows point to the exposed legs of the filter once the right colon and duodenum were rotated out of the way. The duodenum required only a serosal suture. The vena cava above and below the filter and both renal veins had to be controlled to remove the filter which was extirpated in pieces. I have had to do this about once a year or two. The youngest patient I operated on was a 20 year old who had a filter placed after a car accident at 17, but never had it removed. The legs of the filter had eroded into his duodenum causing an abscess.

Iliocaval Thrombosis
The figure below shows two panels with a Trapease filter associated with an iliocaval thrombosis. This patient had cardiovascular collapse and severe bilateral lower extremity edema after a long car ride.
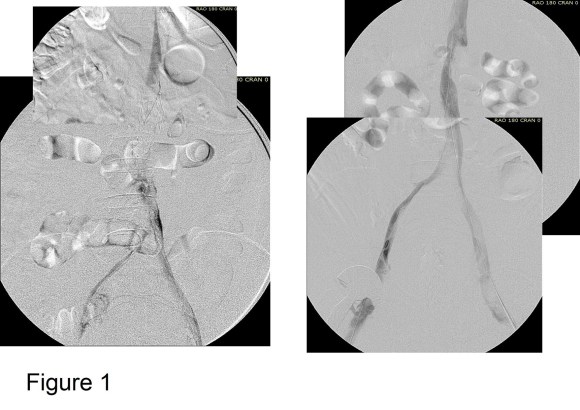
Venography showed iliocaval thrombosis. Thrombolysis was started and the second panel on right of Figure 1 shows the result.
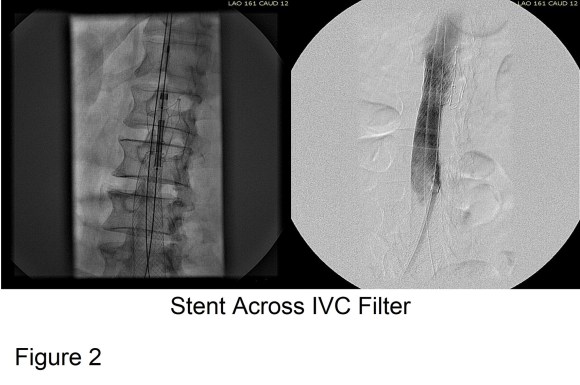
Large WallStents were used to support the recanalized iliocaval system from the common femoral veins to the filter. A Palmaz stent was deployed across the filter (Figure 2).

Figure 3 shows the final result. Interestingly, stents placed across the inguinal ligament into the common femoral vein seem to do fine in contrast to those placed in the artery. IVUS is necessary to confirm good results. Acceptable short term, and durable mid to long term results are reported.
Remove Them While You Can
Filters should be considered a short term therapy to decrease the risk of pulmonary embolism, and should be removed as soon as it is safe. There seems to be no magic time interval beyond which removal cannot be attempted. If permanent filter placement is planned, it should only be for established indications.

One reply on “All Those IVC Filters”
Thank you Dr. Park. I get semi-regular requests to bring in aortic extenders and limbs on days where VC filters are scheduled to be removed…just in case. My older brother had a VC filter placed after a PE and I made sure that it was removed asap.
LikeLike