In George Orwell’s Animal Farm, under the dictatorship of the alpha pig, Napoleon, the pigs who represented the nomenklatura of the farm chant the slogan “four legs good, two legs better,” after initially declaring “four legs good, two legs bad” during their revolution. They clearly understood the luxury afforded by a bipedal lifestyle, because in rising on two legs, you get arms and hands which can do many things like caress a baby or wield a cudgel. What the pigs in the parable weren’t realizing were the consequences of a bipedal lifestyle.
When Lucy, the Australopithecine, bipedal hominid ran about on two legs, she did have the use of two arms and hands. Possibly an adaptation to living in tall grasslands with few trees, the ability to stand tall like meerkats, allowed the biped to see far into the horizon for big cats who probably loved the big brained hominid for the high calorie meal inside the hard skull -many fossils from this time show puncture marks from the incisors of medium to large cats.
The walking and running put heat stress on the brain, and the tool use which happened incredibly early and is observed in the chimpanzee, likely drove the selection for a larger brain (more neurons will allow for one to lose some neurons to heat stress but stay in the game), but it created likely the first problem for our ancestors -discharging a cantaloupe sized head through a pelvis that was small to begin with but now also reshaped for bipedalism. We still suffer from a childbirth process that no other mammal faces -birthing a less than fully cooked baby -a tradeoff for that giant head.
Standing also meant the load bearing was shifted 90 degrees with long term consequences. For our ancestors who only lived about 20-40 years if the chimps are correct, this wasn’t a big deal as arthritis and tendinitis didn’t preclude eating and breeding and didn’t affect them until they were old. But with modern sanitation and social structures, we are reaching 100 years and the majority of the problems of the integument -the bones and ligament, the low back pain, the sore knees, the ratchety hips, can all be explained by our bipedal lifestyle. Your arm is 30-50 pounds of meat and bone and supported only by muscles off your spine, and your blood vessels and nerves traverse a narrow passage through these muscles and your first rib. Your diaphragm with 5-10 pounds of heart, lungs, and blood sits on first branch artery off of your aorta. Your veins, designed to drain blood from your organs, have to do so with over a meter of static water pressure and your sump pumps only work when you are walking. Muscles and their tendons are stretched tight in the odd way that upright walking and running demands, compressing blood vessels and nerves. All of this weight is put on your feet which have to deal with up to a ton of pressure with running…
I’ve talked about this concept many times before but never had a chance to put it together like this talk. I may write an article. Looking back, I did this blog post (Link).
I am grateful to Ms. Mei Nortley and Mr. John Raphael for the invitation to give this talk.
A case report co-authored by my recently graduated trainees, Drs. Roy Miler and Eric Shang. An update to be presented at Midwest Vascular Surgery Society Meeting in Chicago.
The patient is a young woman in her twenties who developed severe right sided abdominal and back pain about 4 months prior to presentation associated with bouts of bloody urine. Activity and standing exacerbated her pain and inactivity and recumbency relieved it. She gained 15 pounds because of her inactivity. Examination was significant for tenderness over her left kidney. Urinanalysis showed positive proteinuria and hemaglobinuria.
Prior to consultation with me she had had an MR venogram showing compression of her left renal vein by the superior mesenteric artery (nutcracker phenomena). The presence of hematuria, proteinuria, and pain (albeit atypically right sided) made it nutcracker syndrome.
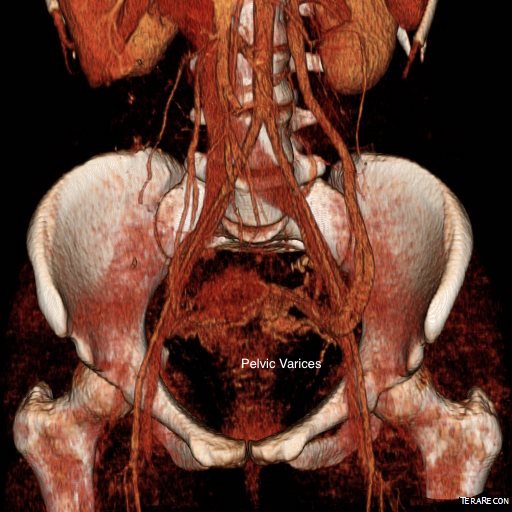
Dilated left gonadal vein and pelvic varices indicate left renal vein (LRV) ouflow obstruction by the superior mesenteric artery (SMA)
I ordered a renal duplex and a CT venogram for procedural planning.
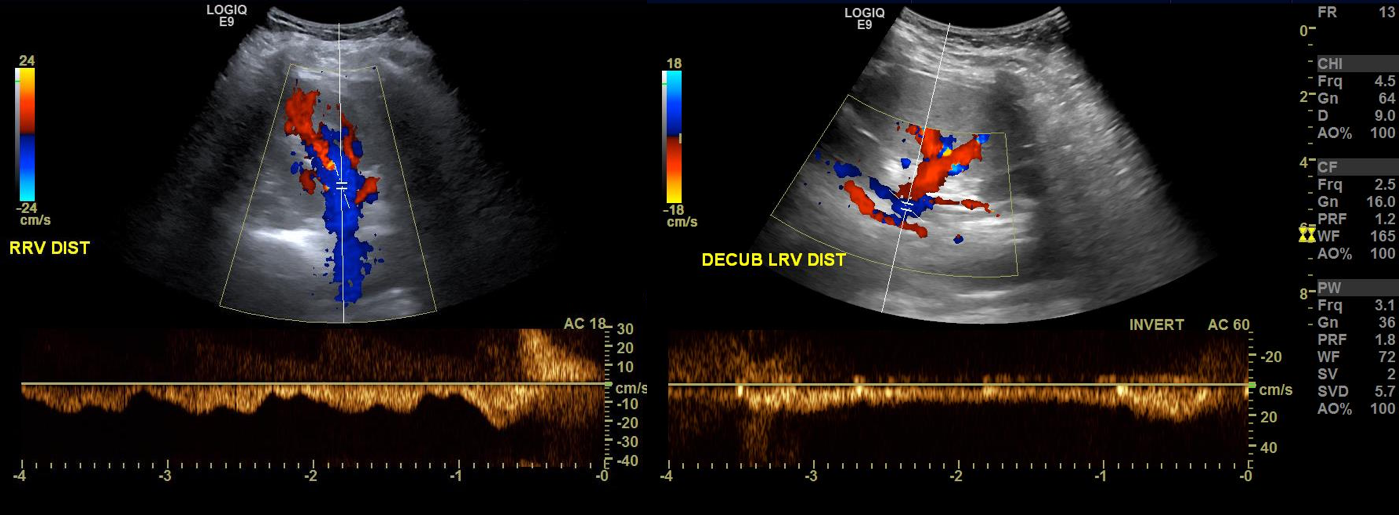
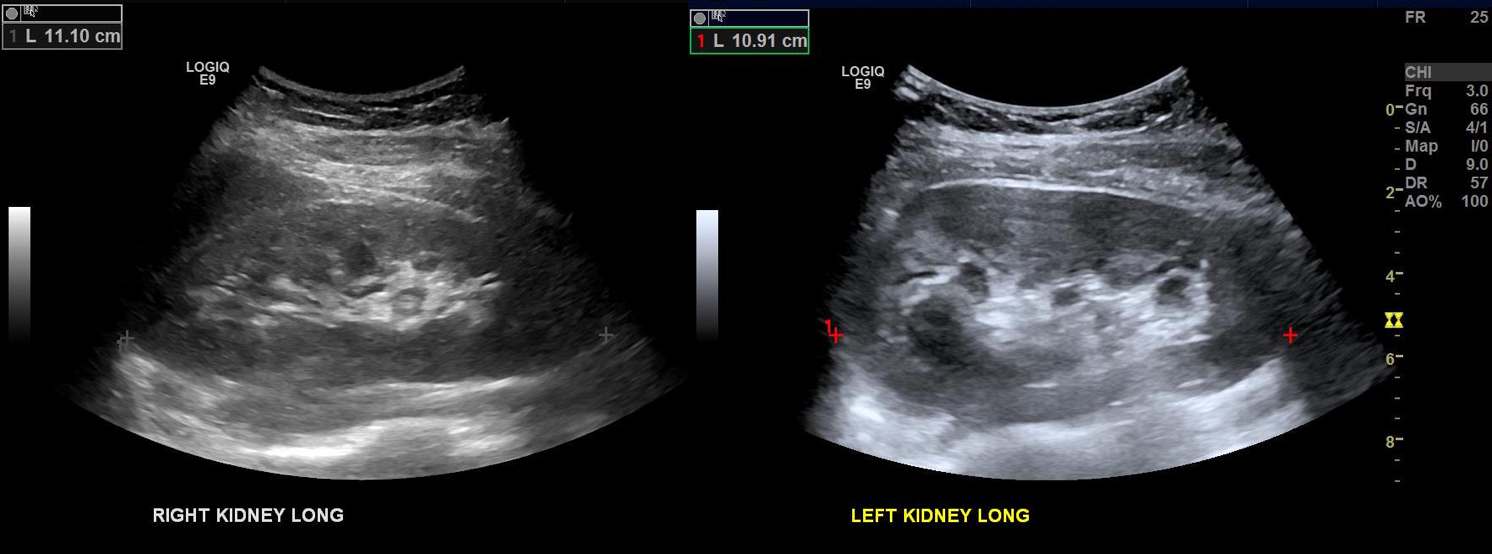
On the duplex, the proximal left renal vein (LRV) was not visualized. The right kidney had normal parenchymal appearance and blood flows, while the left, the kidney appeared distended and had flows consistent with outflow obstruction.
Spectral Doppler flows show respirophasicity in right renal vein(RRV), outflow obstruction on left renal vein (LRV)
The left kidney is swollen and tender.
CT Venography showed the gonadal vein to be an important outflow vessel to the left renal vein with dilated proximal segment and reflux into pelvic varices.
A left gonadal vein to iliac vein transposition was planned via a left lower quadrant retroperitoneal exposure. On the table, a venogram was performed with selective access of the left renal vein.
The injection from the LRV showed severe compression of the LRV with a channel only slightly larger than the sheath and avid reflux into the gonadal vein. Selective access into the gonadal vein and venography from a confluence in the pelvis showed that flow was one way from the LRV into the gonadal vein and this filled a large region of pelvic varices.
The gonadal vein was large caliber and refluxed into two large veins in the pelvis. The one that fed the varices was not selected for transposition, but rather the longer straighter tributary. A catheter was left for easier identification during the dissection.
A left lower quadrant incision was made and a retroperitoneal dissection performed exposing the gonadal vein and iliac vein.
Prior to ligation of the tributaries, a sheath was inserted and through this a LeMaitre valvulotome was brought up to the left renal vein and carefully deployed and pulled back, cutting the valves. This greatly increased the outflow from the vein as evidenced by the height of the blood spout from the vein when the sheath was removed. The varices were ligated at their root -treating them definitively. Transposition was to the external iliac vein, and I could see the feasibility of a laparoscopic or robotic approach to this operation (ref 3).
Completion venography showed excellent flow from the LRV down the gonadal vein into the iliac venous system.
The patient lost less than 10mL of blood and was discharged on postop day 2. Gratifyingly, all of her preoperative pain resolved and her UA showed no more hemoglobinuria or proteinuria.
Discussion
The described treatment options for nutcracker syndrome include (ref 1):
Medical therapy aimed at decreasing renal venous hypertension (for hematuria)
Renal autotransplantation
Left renal vein transposition
Left renal vein to vena cava bypass (autologous or PTFE)
SMA transposition
Nephrectomy
Gonadal vein to IVC bypass
Exovascular stenting (wrap of renal vein with ringed PTFE graft)
Endovascular stenting
Many of the operations are of historic interest. Stenting deserves some comment. The patient self referred because she had read multiple reports of cardioembolization on internet support group comments. The largest nitinol stent (self expanding) available is 14mm. Wall stents in larger diameters are available, but are stiff, poorly conformable, and will elongate if constrained by a non-dilating stenosis like the external compression by the SMA. While acceptable results have been reported, the long term results (20-70 years) for younger patients is unknown. Migration is highly morbid, and usually to the heart, requiring sternotomy and cardiotomy to retrieve the stent. Optimally, a conforming 16-28mm self expanding stent should eventually become available, but conformability is typically inversely proportional to radial strength, and it is the less conformable stents that migrate. Work is ongoing to bring larger diameter nitinol stents for venous indications. The difference between May-Thurner Syndrome and Nutcracker syndrome isn’t merely the size of the veins and stents. The iliocaval confluence is relatively static with some movement of the lumbosacral joints and well suited for treatment with the relatively nonconforming Wall Stents. The left renal vein under the SMA is a very dynamic environment with motion of the SMA and the kidneys with respiration, ambulation, and activity leaving stents vulnerable early to migration and later to fracture.
The left renal vein transposition to the IVC is a nice operation with a good track record (ref 2). The downside is the long midline incision required with transperitoneal exposure. There is bleeding risk and postoperative complications of ileus, wound infection, and small bowel obstruction. Looking at the CTV, it seems obvious that the gonadal vein crosses over the iliac vein in the pelvis and would be a straightforward, less morbid, less invasive option. A review of the literature reveals only a single reference discussing three cases of left renal vein transposition (ref 3), and it was done with a surgical robot. I think that a laparoscopic approach would be simpler and less invasive and will consider developing this if volumes justify it. That said, the open retroperitoneal approach is very straightforward and well used exposure. Using venography to set up and then confirm the results of the transposition was helpful. I don’t think that measuring pressures and diameters and taking calipers to calculate stenoses is all that useful and in some instances a harmful method of justifying endovascular treatment of nutcracker phenomena in the absence of serious symptoms and a careful deliberate workup which includes a good history and physical, a UA, a duplex and CTV.
Intervening on the gonadal vein to iliac vein anastomosis should be straightforward from a groin or thigh venous access on the ipsilateral side. This operation doesn’t preclude any future interventions on the LRV. The pelvic varices were treated with direct ligation. The patient’s pain was successfully relieved in the short term.
Conclusion: Open retroperitoneal left gonadal vein to iliac vein transposition with gonadal vein valvulotomy is effecting in treating nutcracker syndrome.
References
Kurklinsky AK, Rooke TW. Mayo Clin Proc. 2010 Jun; 85(6): 552–559.
Reed NR et al. J Vasc Surg. 2009 Feb;49(2):386-93;