VESS is a special medical society whose mission is to foster academic activity and collegiality among young vascular surgeons. Dr. Vikram Kashyap, the outgoing president, gave an engaging talk about changing with the times, referencing three powerhouse rock groups -Rush, The Police, and the Red Hot Chili Peppers, three of my favorite groups.
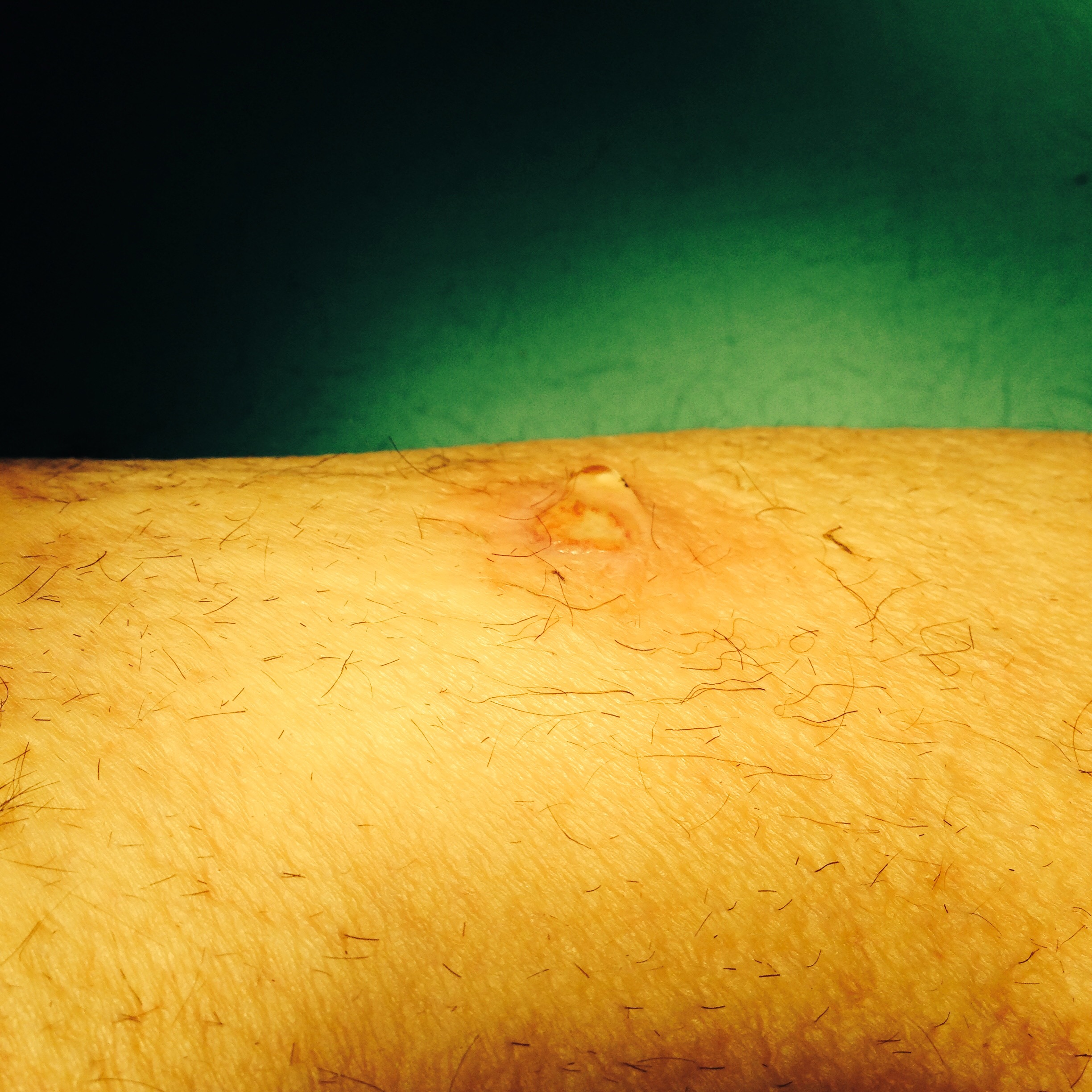
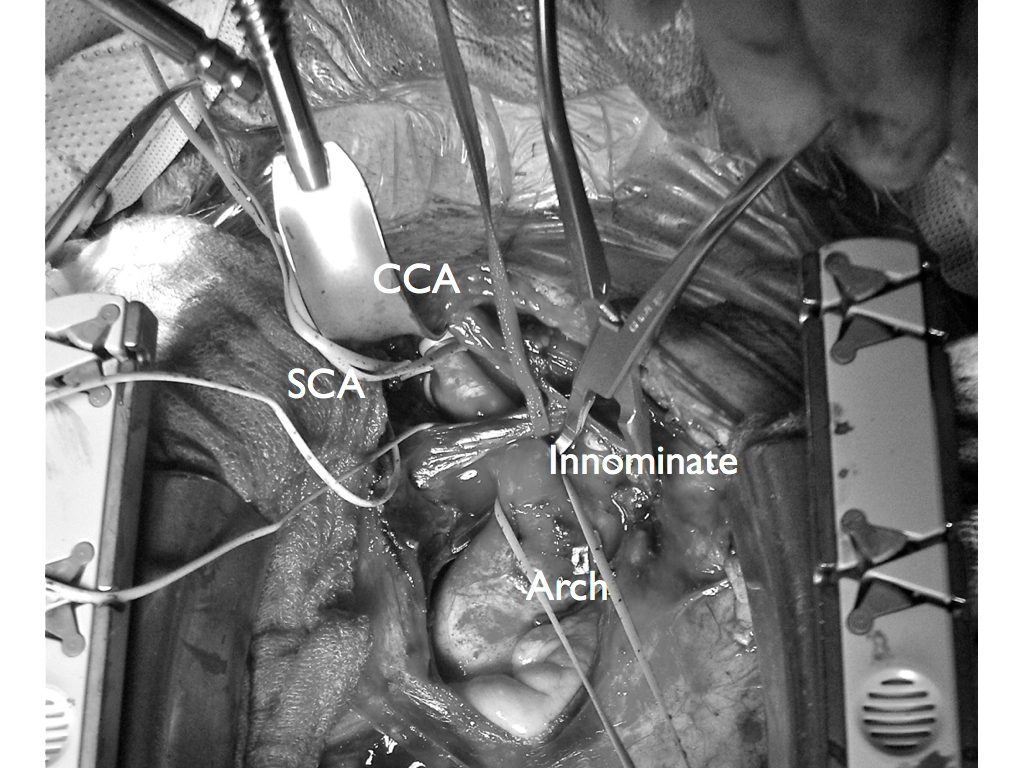
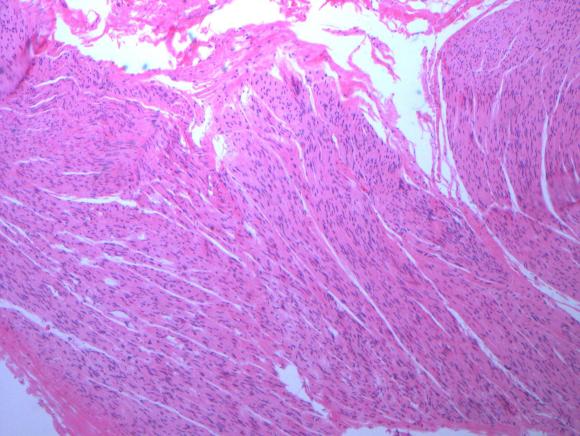
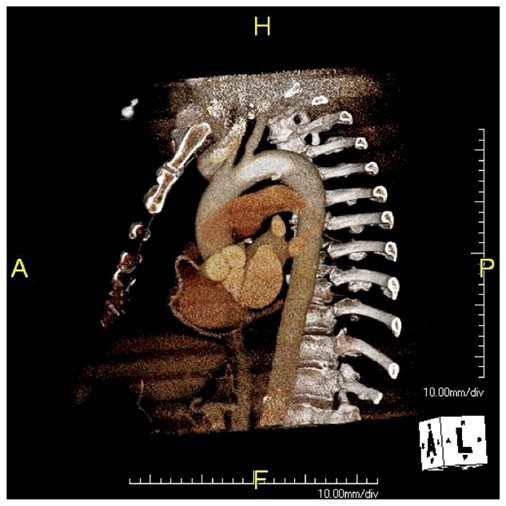
Dr. Max Wohlauer presented our case report on “Osteosarcoma masquerading as an axillary artery pseudoanuerysm.”
The case report ended the Friday morning session and was well received.

Dr. John Weber opened the Friday afternoon session with “Median arcuate ligament syndrome is not a vascular disease.” Shown above prepping for the talk, he is also in the conference dress code of being ready for the slopes.
The talk was also well received and not surprising to most who agreed. In a conversation I had with Dr. Kenneth Cherry, he mentioned that he and Dr. Jeb Hallett had concluded as much decades ago.
The scuttlebutt in the conference was about the NY Times article about the scandalous overuse of femoral stents by some physicians. It is a matter of course that the first line of therapy for mild to moderate claudication is a combination of risk factor modification and exercise therapy -something not mentioned by the writers as something emphasized by Vascular Surgeons who as a rule are against plying stents on asymptomatic or mildly symptomatic patients.
The other thing was the tremendous demand for vascular surgeons, and the success of the 0-5 training programs which represent the future of vascular surgery. Dr. Karl Illig professed as much in the Q&A of a report from Wake Forest. Surprisingly the majority (100%) of 0-5 graduates in 2013 went into academic practice.