Dr. Roberto Chiesa from Italy presented his experience in 61 renal arteries using the Gore hybrid graft today at the Veith Symposium The graft which I sketched above on my phone is their PTFE graft terminated in a Viabahn configuration. He reports a 10% acute renal failure rate and 90% primary patency in followup. This is something I’ve considered but never tried because the one extra anastomosis doesn’t add all that more time especially if a branched graft is used. Will revisit this concept.
Dr. Debus presented using this graft in a later talk for debranching visceral arteries in hybrid repair of TAAA.
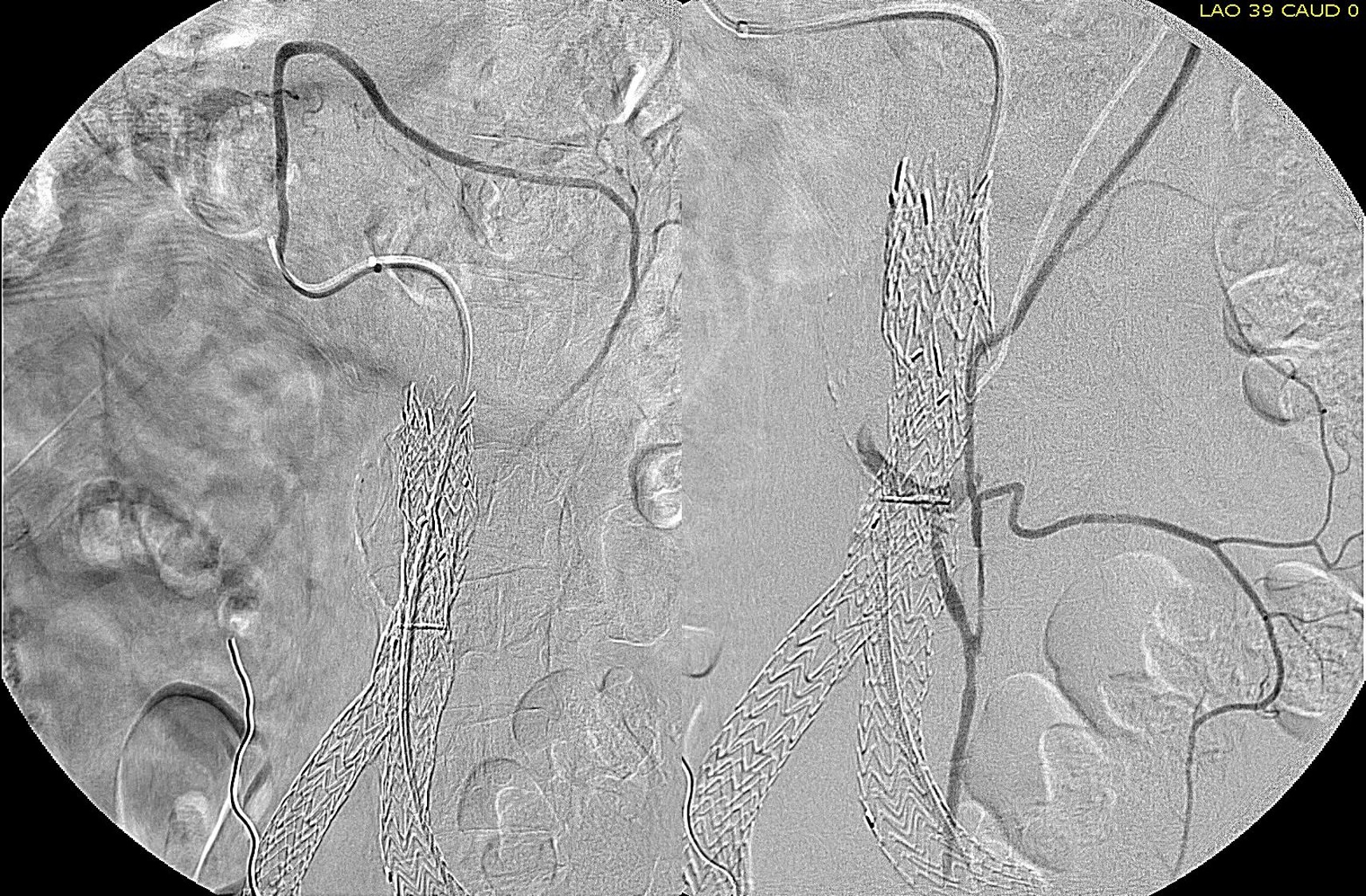
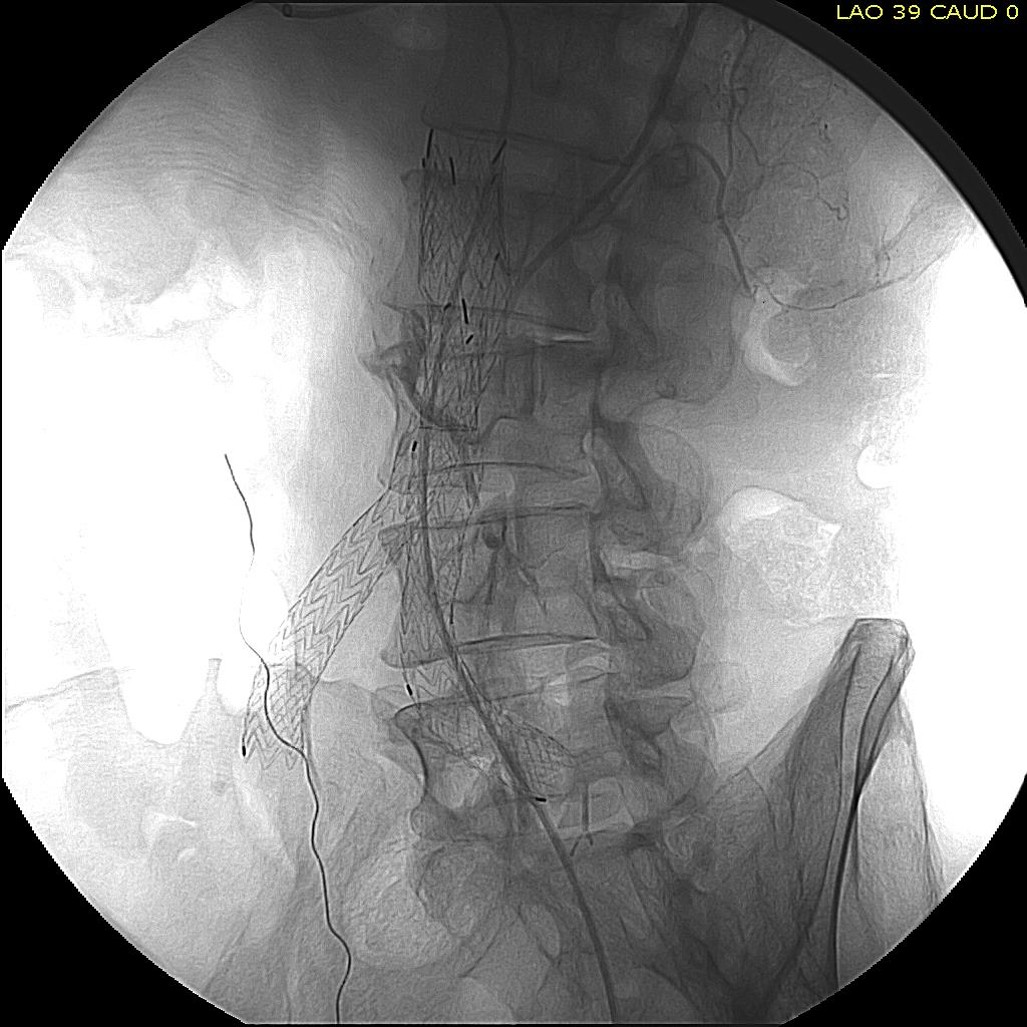
This patient presented with abdominal pain and found to have a 9.5cm AAA. CT showed a previous stent graft that had slipped its moorings from a very short neck, and had actually flipped down on itself.
The patient was a very sick man with an AICD, end stage CHF, and severe COPD on home O2, and had been turned down for a heart transplant. He relayed that surgeon who had performed the EVAR 6 years before had informed him to follow up with his primary care physician.
This patient was repaired with an AUI-Fem-Fem with plug occlusion of his left iliac. The patient recovered and was POD #6, to his home.
November 13, 2014
This was not the first patient I had like this. Pictured below is another patient with a similar scenario from my personal photo bank. It is important to understand that aneurysms are dynamic, particularly if tortuous. Many of the early generation grafts were placed with great enthusiasm in all sorts of anatomy and they come back to us. Here at the clinic, Dr. Eric Turney and others reported that from 1999 to 2012, 100 patient required EVAR explant. Overall mortality was 17%, with an elective case mortality of 9.9%, non-elective mortality of 37%, and 56% mortality for ruptures (reference). Excluding the 13% of cases that were infected, progression of aneurysm disease was identified as the cause of late (>5yr) failure. It is a major source of open aortic experience for our trainees.
Illustrated below is the mechanism for loss of primary seal when there is a great deal of anterior bowing. Technically, anchoring mechanisms in modern grafts have worked to prevent or delay this effect, but it is something to consider in tortuous anatomy.
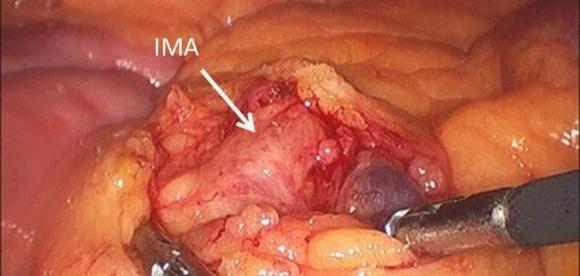
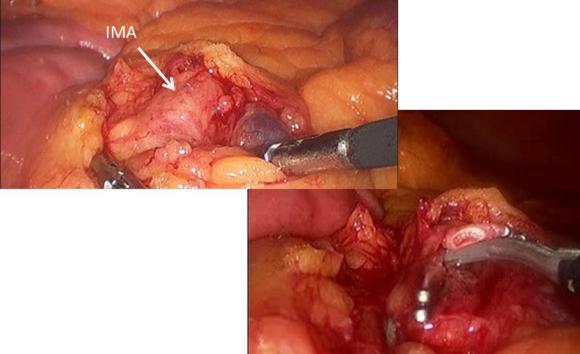
As I had discussed earlier posts, endoleaks can be managed with superselective endovascular access of the AAA sac via the hypogastric artery (Link) or the superior mesenteric artery (Link), but in fact, it may be very easily treated with direct ligation. This patient had a Type II leak causing sac growth from an IMA source and I chose to treat this laparoscopically. The patient was placed in a right lateral decubitus position to use gravity to move the small bowel away from the aorta. An umbilical and left midaxillary line port were placed after pneumoperitoneum was induced. The view above shows the IMA which is readily seen in the retroperitoneum. Ligating it with clips effectively closes the endoleak.
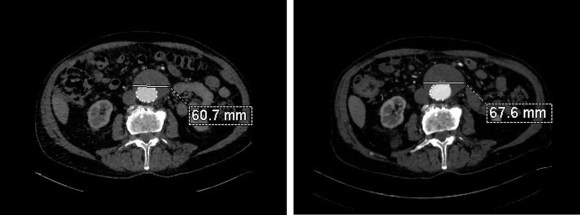
The before and after CT scans show that the endoleak resolves after ligation. This takes about 15-30 minutes of operating.
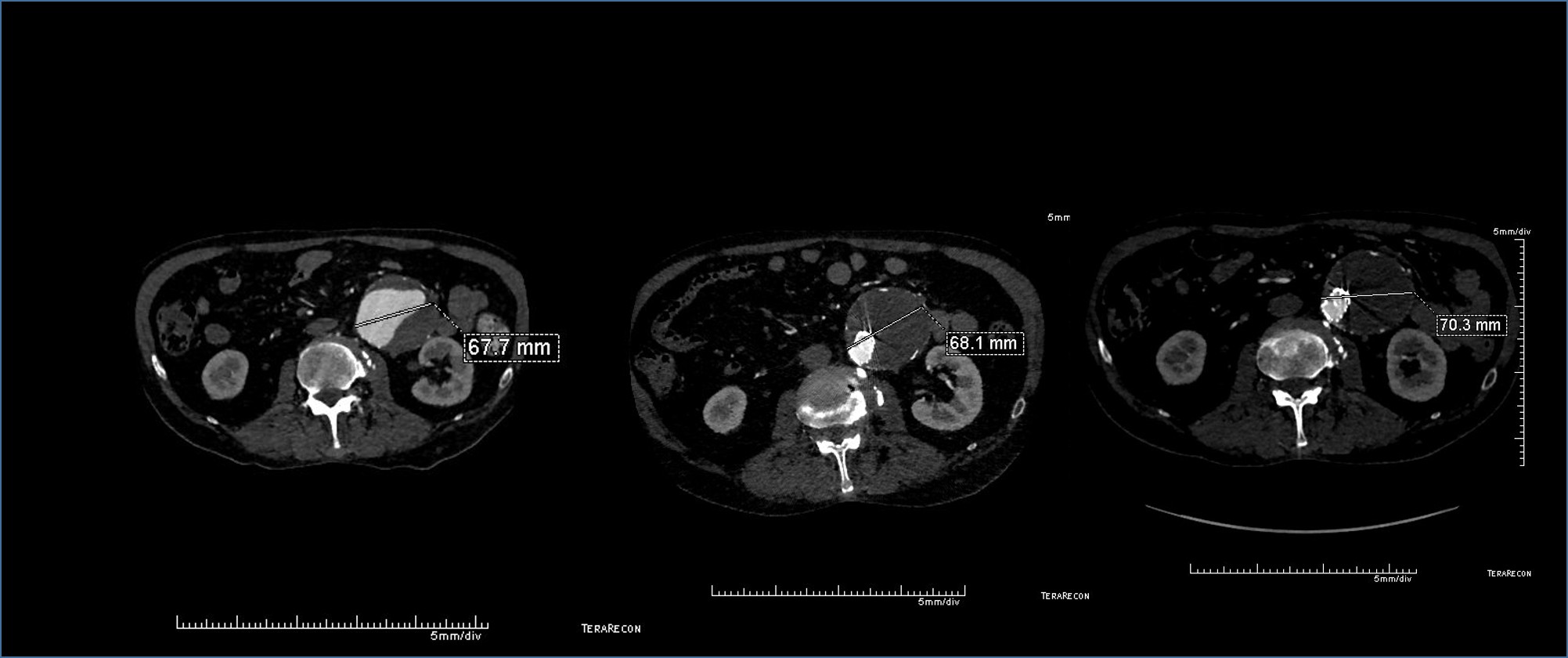
The patient had a successful EVAR or an eccentric infrarenal AAA which in followup grew due to the presence of a type II endoleak from the inferior mesenteric artery. This was seen on the CTA and duplex ultrasound. Planning for assessment and treatment involved analyzing the CTA in centerline, tracking the source of the arterial blood flow into the sac.
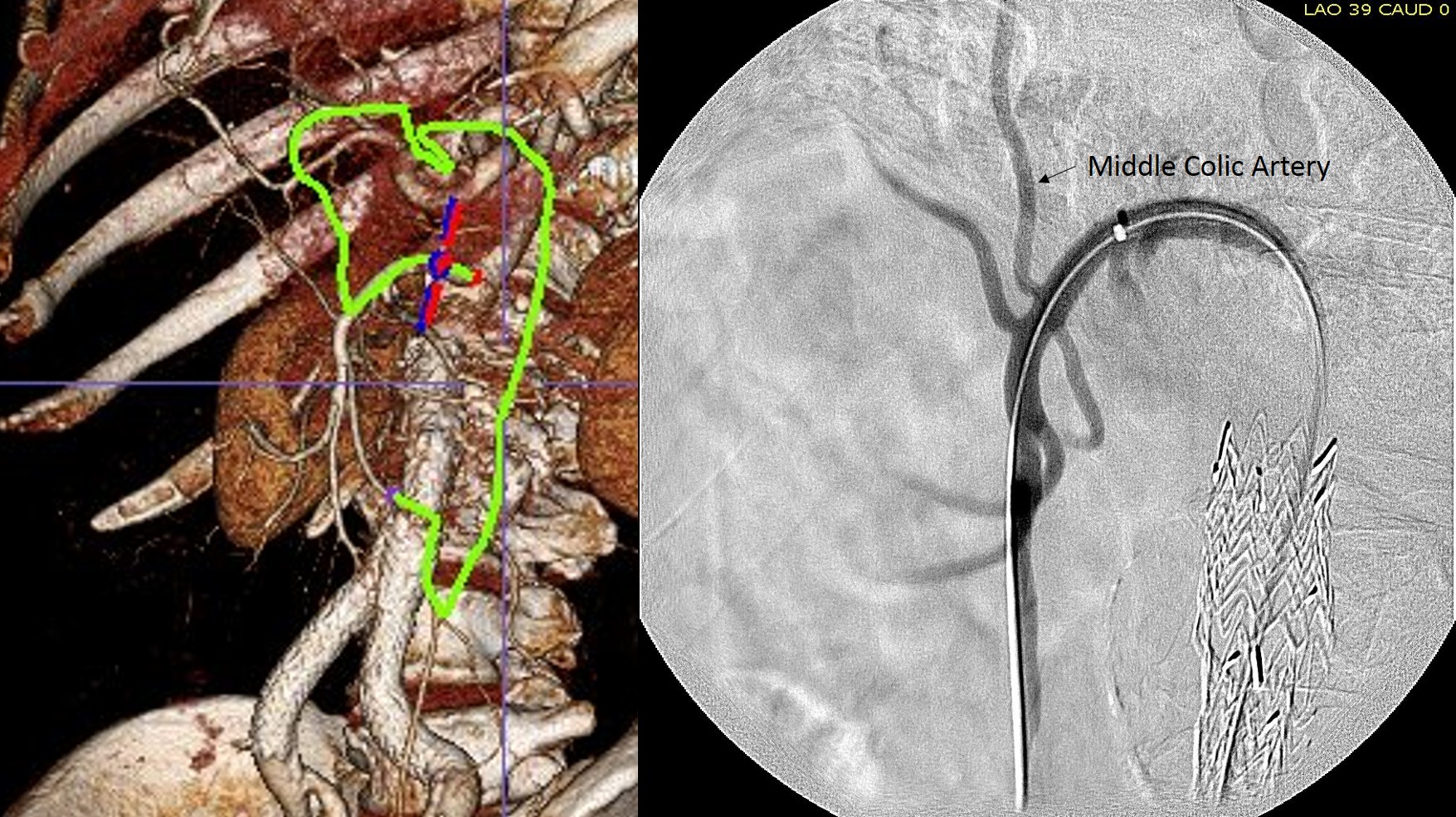
The centerline from the SMA into the middle colic artery shows a meandering but patent path via the Arc of Riolan to the left colic artery to the inferior mesenteric artery. In my experience this is straightforward to access selectively from the femoral approach, but it illustrates for the trainees the concept of building up access which I refer to as building the intervention machine.
The first step in the access involves getting stable footing in the SMA. Selective access can be performed with a shaped catheter, and once accessed, a Rosen wire is used to track in a curved long sheath. Parking this sheath in the proximal SMA forms the foundation of this machine. The next step is access into the middle colic artery.
The CTA is particularly helpful in identifying the middle colic on the 3DVR projection. Selection of this is straightforward with a an angle catheter which I place a Tuohy Borst connector. This is the second stage of the machine, because further access with 0.35guage wires and catheters could result in spasm. This second sheath access (the Tuohy turns the catheter into a sheath) of the middle colic allows for selective 0.18 gauge catheters and wires to make the final step to the IMA and the AAA.
Selective access of middle colic artery (left) and later phase showing IMA and endoleak (right)6F Ansel Sheath in SMA, Angled Glide Catheter into Arc of Riolan, 0.18 Glidewire and catheter in IMANBCA glue used to seal endoleak and IMA
The embolization with NBCA sealed the IMA and the cavity in the AAA sac. This was checked with intraoperative duplex, done with a transabdominal aortic probe.
Before embolization
Transabdominal aortic duplex is easier on sleeping patient and potentially gives more information than arteriography alone. The patient in followup had no endoleak and demonstrated sac shrinkage.
The access machine concept is important for planning interventions. Every major branch or turn needs to be crossed by your ultimate access sheath, if you want to avoid having to arduously reaccess those points, and building up a telescoping layer of sheaths is very handy. Every interventional case is done at some distance away from the access point on the skin, and so some though has to be given to how you will build that machine.
With this example, I have shown that you can readily access the AAA sac from the SMA. An earlier article showed iliofemoral access via the hypogastric artery (link). I will give in an upcoming post how this can be done laparoscopically in under 20 minutes.
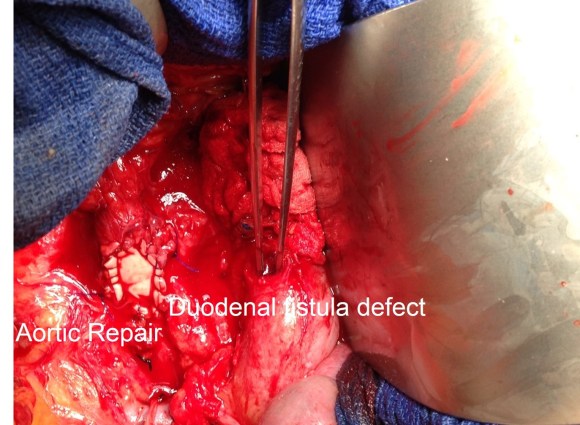
The call came through our transfer center. At the time this patient was transferred, one of the chairmen emeriti of the clinic, called my cell phone with the story. It was still my first year at the clinic and pleasant to be talking to one of the giants of vascular surgery. The patient was suffering from upper gastrointestinal hemorrhages, and not responding to EGD. He was taken to the operating room by his local general surgeon, who soon found that he was bleeding from a primary aortoduodenal fistula. He was able to control the bleeding by putting his finger on the hole but his institution was not set up for vascular surgical care. After a brief conversation, our quarterback decided the patient needed to come rapidly by helicopter with his surgeon maintaining hemostasis –like the proverbial Dutch boy with his finger in the dike. The patient was prepared for transport by placing drapes over his open abdomen with the surgeon maintaining finger pressure on the duodenal fistula, and they arrived like that into the operating room for emergency surgery. The operation was made difficult by inflammation, but I was able to get a clamp on the aorta infrarenally and dismiss the real hero of the day, the patient’s first surgeon who got a helicopter ride home. The aorta was focally necrotic and this was sent for culture which came back MRSA, but otherwise it was normal. I repaired with a bovine pericardial patch and after repair of the duodenum by our general surgeon, omentum was laid down and secured over the aorta and beneath the bowel.
The patient had a history of sarcoidosis and aortic valvular endocarditis, but it was relatively remote. There was no significant atherosclerotic plaque nor aneurysm to account for the development of the aortoduodenal fistula. The patient survived and is doing better now over a year after his rescue by his flying surgeon. The other hero, of course, is the pedicled omental flap. The omentum is a mysterious organ to me and without adequate study or explanation from a functional, developmental, or evolutionary point of view.
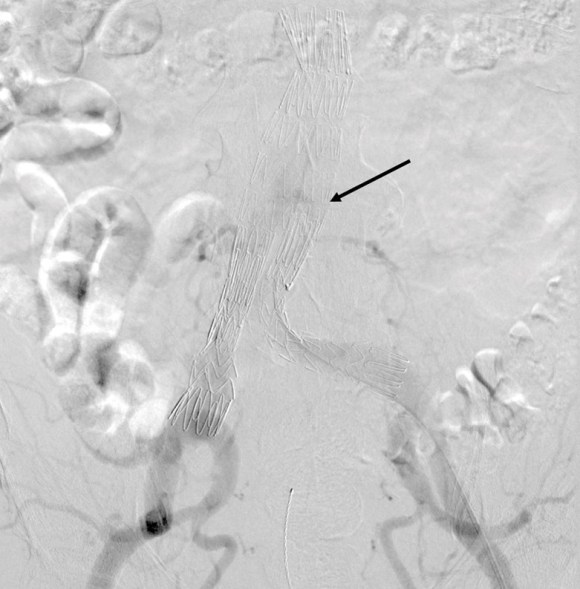
The patient had undergone an uneventful EVAR, but in followup had developed AAA sac growth. Pictured above are the post deployment CT’s from 1 month and 6 months. Reviewing the original aortogram, you can see that there was flow into the sac very late via an iliolumbar collateral.
Plan was made for arteriography and intervention. As discussed in an earlier post, 3D VR was very helpful in planning access to the type II endoleak, particularly in plotting C-arm angles and access vessels.
The 3D-VR image view on Aquarius Intuition (TeraRecon) predicts a camera angle of 50 degree LAO to see the branch leaking to the lumbar vessel causing the leak.
Initial aortography confirms the absence of a type I or III leak in early phase.
Later in the phase, the endoleak can be well seen, corresponding to the CTA.
I do an intraoperative transabdominal duplex of the aorta. I have submitted this technique for presentation and eventual publication, but briefly, using an abdominal probe on the abdomen, the sac and endoleak can be readily visualized, and the source of the leak confirmed.
The inferior mesenteric artery which is so often involved is not in this case, and can be easily seen with duplex in patients who are NPO and under general anesthesia. I perform these studies myself, as they are far less challenging than when a patient is awake.
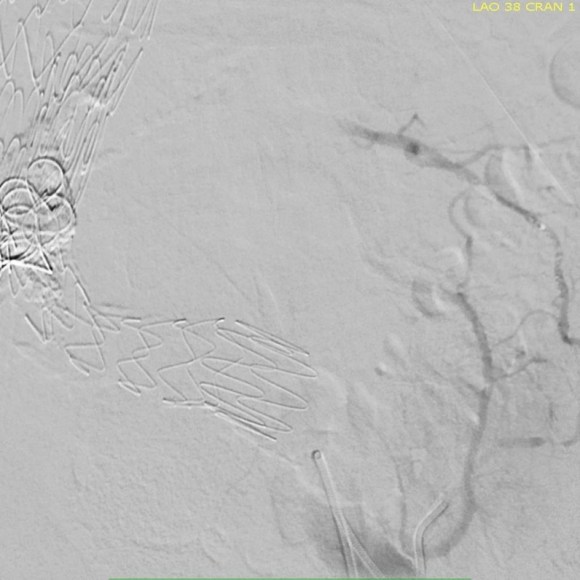
Selection of the branch vessel is straightforward as the CTA well illustrates the course of the source iliolumbar vessel. The CTA even showed the loop that was challenging to traverse. The sequence of access involved IIA, branch access with a glide catheter, placing a Rosen wire for anchorage, and pushing the sheath over the glide catheter into the branch vessel, giving stability. Further access into and across the loop was then possible with superselective catheters based on an 0.18 wire system.
Once access into the AAA sac was achieved, coil embolization of the leak cavity chased by glue (NBCA) allowed for obliteration of the endoleak.
Duplex ultrasound confirmed effective closure, with absence of perigraft flow.
Using duplex in this fashion adds another dimension to the treatment imaging and has the potential for reducing radiation dose and contrast volume.
The patient in followup has shown sac shrinkage. The other treatment options are: direct lumbar puncture, open surgery with sac marsupialization and oversewing of leaks, and laparoscopic ligation of lumbar arteries. I have tried all of these, but this went as easy as could be expected and I credit the ability to visualize the entry path in 3 dimensional virtual reality. The toughest part was negotiating the loop, but a shaped 0.18 glide wire simplified this.
In 2006, Sheehan et al [J Vasc Surg 2006;43:657-61] reviewed an 7 year experience from 5 academic centers. 1909 patients had EVAR with various endografts, and there was an overall 15% rate of type II endoleak. Most resolved within the first year. No significant variation by endograft design appeared to correlate with type II endoleak, which makes sense, although TALENT graft had the highest rate. Spontaneous resolution was common. Late endoleaks were frequent. No conversions were due to type II endoleak. Higashiura, Greenberg et al [J Vasc Interv Radiol 2007;18:975-981] reviewed the CCF experience with the Zenith graft and type II leaks. Of 204 patients with suitable followup, there was a 17% rate of early type II endoleak. Of these, only a 7 of 18 patients with persistent leak developed sac enlargement. Most type II endoleaks spontaneously resolved in followup. No variables could predict persistence of type II endoleak. Treatment prevented sac enlargement.
Silverberg, Marin et al [J Vasc Surg 2006;44:453-59] found similar rates of type II endoleaks -16%, in a study group of 965. Spontaneous resolution occurred in 36% in a mean time of 14.5 months. Treatment was reserved for sac enlargement. 8.4% of those with type II endoleaks experienced sac enlargement greater than 5mm. The vast majority of patients had a benign course. Regression analysis revealed cancer, CAD, COPD were associated with earlier spontaneous closure of type II endoleaks.
Ruptures can occur with persistent type II endoleak [Jones, Cambria et al. J Vasc Surg 2007;46:1-8]. Selective treatment of those with persistent leak and sac growth >5mm seems to be a safe and cost effective approach [Steinmetz, Sicard et al. J Vasc Surg 2004;39:306-13].
Percutaneous access for EVAR and TEVAR does several things. First, the procedure becomes shorter by an hour or two, and (don’t discount not having nursing count instruments because the case was percutaneous). Second, the patients experience far less discomfort and it is easier to discharge them the next day when they have a bandaid versus an incision. And this leads to the third thing: not having an incision means it is far less likely that a groin infection will occur, especially in the obese.
There are three things which you must do before undertaking pEVAR. First, you have to become comfortable with using the Perclose S device in 6F-8F access -about 5 to 10 successful closures will do. You should become facile with the deployment of the sutures and closure of the access point. Avoid small arteries or heavily calcified arteries. This leads to the second point -all of your groin access should be ultrasound guided -this has been shown to improve results in pEVAR (Ref 1). I am a firm believer that the source of groin access complications starts with the initial needle stick. The 18g needle is basically a short 11 blade rolled up into a cylinder, and during groin access without ultrasound imaging, one can shear branch arteries, skewer arteries, dissect plaque, and access too proximally or distally, or into the profunda femoris.
The third need is access to 3D reconstruction software and multislice CTA. This gives you powerful ability to predict which patients are more suitable for a percutaneous approach, and which should have a cut down, and with 3D virtual reality reconstructions, you can plan where the incisions will be. In the skinny patient, this is not a pressing issue, but in the merely obese and the frankly obese, and the super obese, choosing to go percutaneous and avoiding a groin complication, which may be the one thing that debilitates the patient far more than a stent graft deployment, becomes an easy decision with experience.
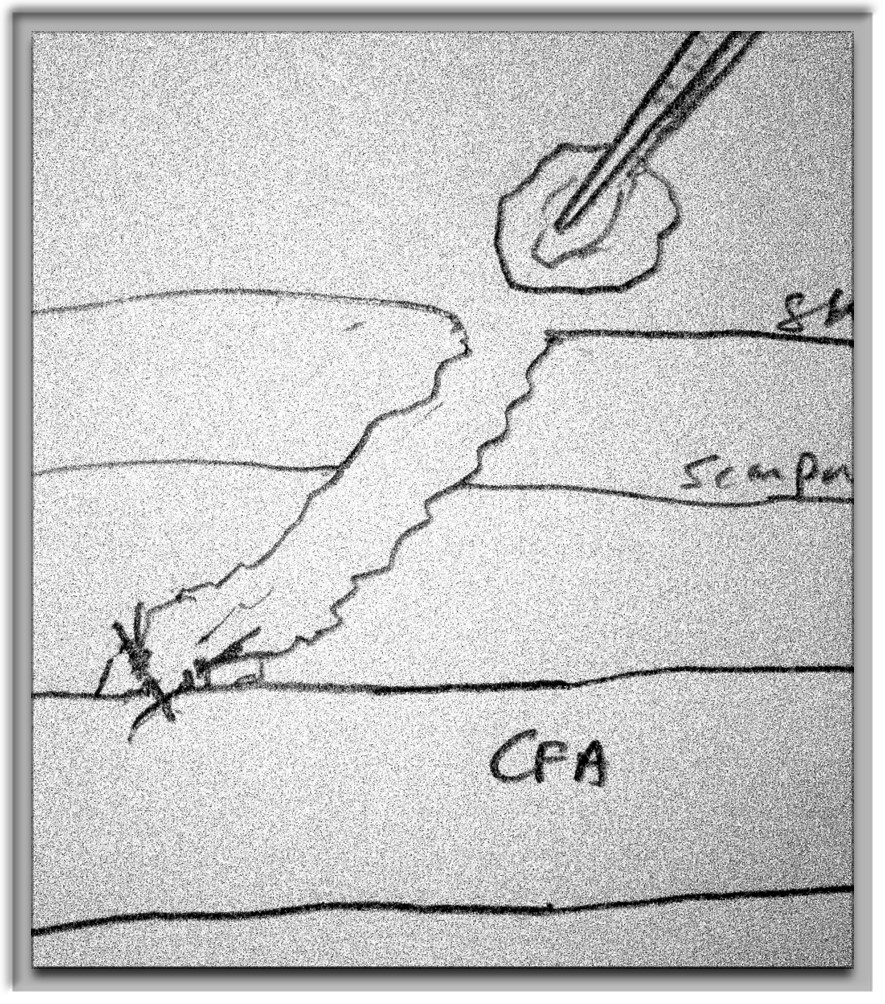
As you build your 6-8F Perclose experience, you may notice that having too tight and subcutaneous tract can result in the suture catching on SQ fat, and not closing, or that bleeding won’t surface properly and create a hematoma under Scarpa’s fascia, often after the patient gets to the recovery room. Expanding on this principle, as you leap to 12F access and preclosure, I recommend you try this -make a 10mm incision, and using a tonsil clamp, pop through Scarpa’s fascia and seat the tips of the clamp under ultrasound on top of the soft part of the CFA that you intend to access. Gently spreading creates the space that you need to deploy the sutures and ensure that any bleeding will exit the skin and not dive under the fascia. It amounts to an ultrasound guided dissection of the common femoral artery. Before you remove the tonsil, you gently maneuver a micropuncture (always) access needle between the tines of the tonsil clamp until it gets to the artery -this keeps the eventual wire going through the tunnel you just made.
12F can usually close with a single Perclose, but start practicing by placing two Perclose sutures in a 10 oclock and 2 oclock orientation. Once the sutures are in, I make sure the two ends of the suture are pulled out and the end loop of the suture is on the artery and I clamp these sutures to the drapes medially and laterally depending on how I deploy the two sutures. This also helps avoid catching the suture and driving it into the aorta.
After performing EVAR or TEVAR, I remove the sheath, leaving a wire -typically the stiff wire originally supporting the sheath and deploy one of the sutures. This first suture should cinch down onto the artery and substantially decrease the bleeding coming from the access site. I then deploy the second suture, and if the bleeding has stopped or is a steady dribble, I remove the wire. If pulsatile bleeding persists, I recinch the sutures using the knot pushers. If this decreases flow, I remove the wire, otherwise, I place a dilator, stop the bleeding and cut down. Cutting down after SQ dissection means merely dividing skin and tissues over the dilator, and the artery is easily visible for suture placement. If I remove the wire and there is still some bleeding, and usually there is, I place Gel-Foam soaked in diluted thrombin into the tract, reverse heparin, and hold pressure for 10-20minutes. It is very rare to have to convert after this is done.
thrombin-gelfoam into tract
The skin is closed with an absorbable 4-0 monofilament suture, and skin glue. I usually use the micropuncture needle to give an ilioinguinal field block with Marcaine. This gives 24hrs of pain relief.
A note about incisions. Usually, with 3D VR imaging of CTA, the CFA and its quality (size and absence of plaque), and location relative to the inguinal crease can be ascertained. I try to make the access point at the inguinal crease or distally, as this goes under the subpannus of groin fat rather than through it.
3D-VR imaging can pinpoint optimal access
I sincerely believe sheath size is not the limiting factor to percutaneous access. Rather, it is the common femoral and iliac artery. Zakko et al at the University of Florida just published their experience on the obese with percutaneous TEVAR (ref 2), and found that while the arteries were deeper, the technical success rate of staying percutaneous (over 90%) was no different between their obese patients non-obese patients. The predictors of failure were poor access artery quality and size. I believe that you can select for patients most likely to succeed and greatly reduce failure. In this population, groin complications are potentially life threatening, and avoiding an open groin exposure is valuable.
Here is a link to the current issue of Cardiac Consult where I have a case report of a difficult EVAR. In it also is a feature on our vice chair, Dr. Timur Sarac, and his bioabsorbable stent, and Dr. Eric Roselli of the Cardiovascular Surgery on stent grafting of ascending thoracic aortic dissections, for which he received special recognition at todays State of the Clinic address by Dr. Cosgrove.