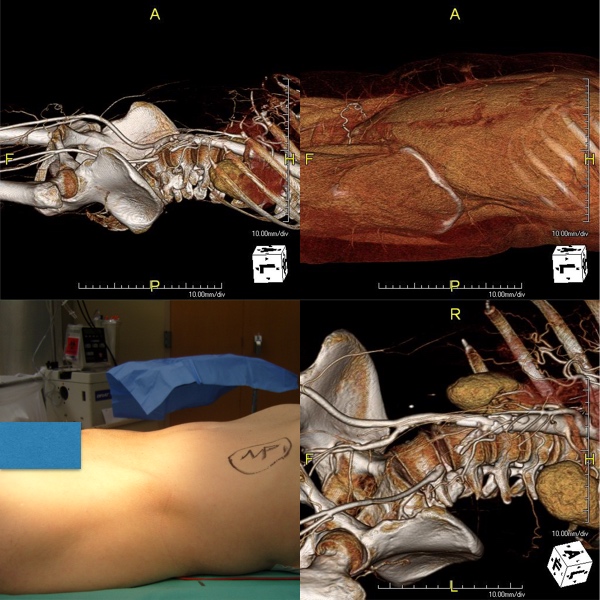
The images above show a patient with on isolated occlusion of his left common iliac artery. He was young, in his forties, but was a heavy smoker and suddenly developed claudication of his left leg which interfered with his work. He quit smoking and did not progress with exercise. Discussion involving possible stenting was made and initially offered but he turned it down because erroneously he assumed that his father’s coronary stents were the same as an iliac stent in terms of longevity. I do think that common iliac and aortoiliac occlusive disease is well treated with stents, but I felt it was possible to do a common iliac endarterectomy. We went over these images together and he settled on proceeding with endarterectomy.
The images show how well the 3D Volume Rendering, which I mentally call Virtual Reality, of CTA makes it possible to plan out operations and exposures virtually. The bottom left image shows the surgeon’s eye view of the exposed vessel.
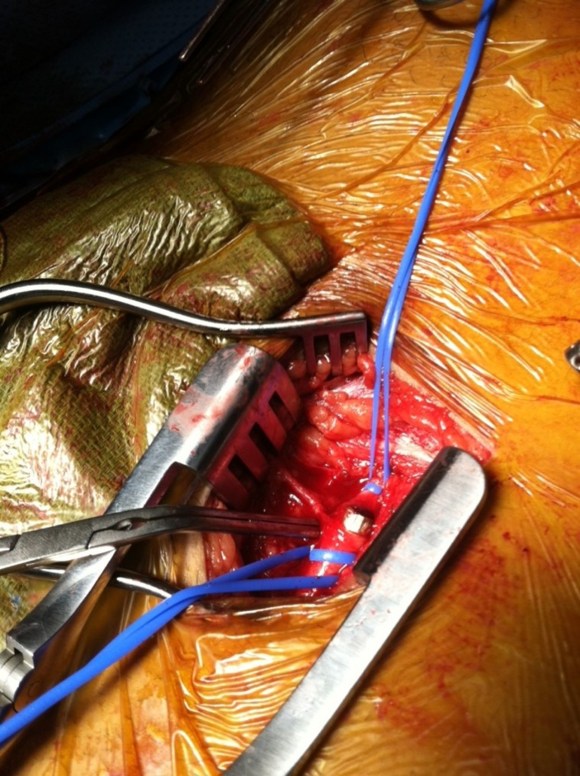
Below, the virtual and the actual are juxtaposed.
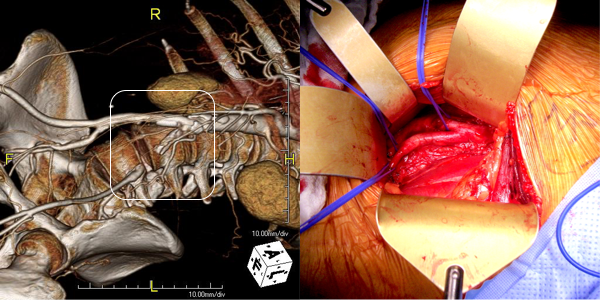
The outline on the virtual image (volume rendered) shows the areas of retraction -for the trainees, the retractor systems work to make quadrilaterals out of linear incisions, and as a rule, the incision should be twice the length of the square that you want to expose. The end points of the endarterectomy were at the aortic and iliac bifurcations.

The arteriotomy was repaired with a patch at the iliac bifurcation -the common iliac was large and was repaired primarily.

The specimen below was fibrocalcific. The thing about this disease is that the plaque truly has no endpoint -intimal thickening and mild plaque was present that could be taken all the way to the aortic root and to the feet on the other end!

This patient did very well and had palpable pulses. He did not develop neointimal hyperplasia and successfully quit smoking.
One of the exciting developments is the ongoing development of wearable virtual reality and display solutions -particularly from the gaming industry. The gaming industry ironically drives all computer imaging because that is where the money is at. The advances in imaging trickle down to medicine -the VR images seen here are the result of the same algorithms that drive first person shooting games. It would be great to see this displayed intraop on a HoloLens, on a virtually positioned screen behind the assistant!