Before manufactured thoracic stent grafts were approved for use, you had to make your own. I think that even in theory you should have this in your mental locker, because it is pretty straight forward to accomplish. The patient was a homeless man who got struck by an SUV while crossing Broadway merely blocks from Columbia Presbyterian. The specifics are lost to time, but he was found to have among his multiple injuries a tear in his thoracic aorta at the ligamentum arteriosum. Cardiothoracic surgery felt that he was far too high a risk to undergo open repair. I was on call, and when I looked at this patient’s scans, I realized that he might survive with a stent graft across the tear, but the only suitable grafts were short aortic cuffs intended for infrarenal repair with short delivery systems. Being young staff, I called our site chief at that time, a grizzled veteran, for some advice about making stent grafts.


The process is simple enough, and discovering it is like finding out that a seemingly complicated dish has an exceedingly simple recipe. The process starts with an iron and an ironing board, with which you press flat a Cooley graft of 32 or larger diameter. The Cooley graft is a fine weave graft that has pressed cylindrical folds that allow you to collapse it like a Slinky toy. Ironing between two sheets of paper allows you to avoid overheating the fabric.

Once flattened and stretched, it is now ready for placement of stents. The stents shown here are Gianturco stents which typically are constrained with a monofilament and has barbs. The barbs are removed with needle nose pliers. 5-0 monofilament suture is used to secure the stents in the graft. More spacing allows for the graft to accommodate tortuosity, but the graft may bunch up in the sheath. The top and bottom stents should be within 5mm of the graft edge –this way you will remember that at deployment.

For this case which required only one stent, three were made and they were autoclaved. Loading into a large sheath of 24F is done over a catheter to preserve a wire channel. The graft is pushed in using the umbilical tape or silk suture technique referenced in Oderich’s paper about reloading modified stent grafts.
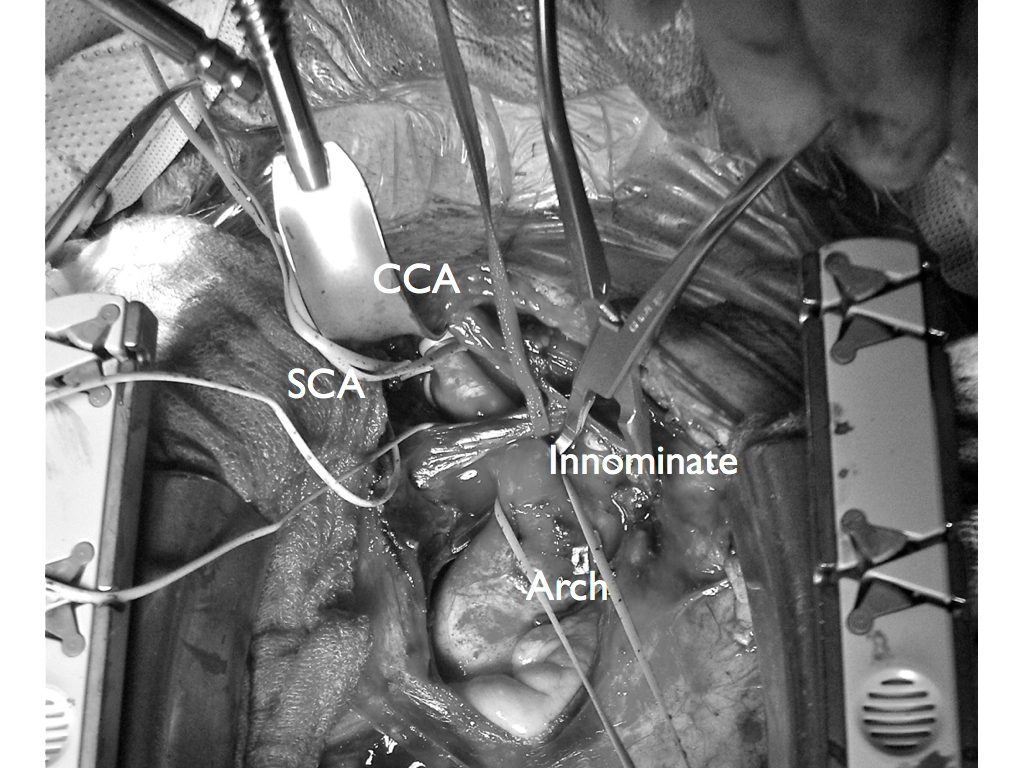
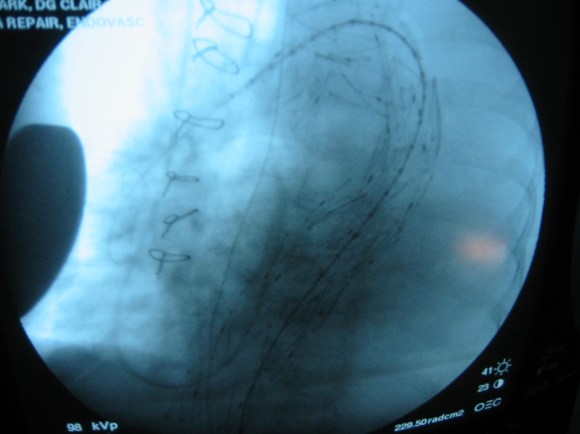
Because of the large deliver system, a conduit was required and sutured end to end into the common iliac artery –I no longer do this unless there is a problem with severe plaque requiring endarterectomy. The graft was deployed by push-pull technique with the heart rate slowed pharmacologically. The patient stabilized from this, took several months to recover from his other injuries but was discharged and lost to followup.


Is this knowledge helpful? In 2015, debatable, but in 2003, it saved a life.