

The patient severe claudication and nocturnal rest pain and had undergone an inflow procedure at another hospital consisting of a common femoral endarterectomy and a single stent to the external iliac artery near its origin from the iliac bifurcation. He also had undergone a concurrent SFA atherectomy which closed and was treated with SFA stents extending from the SFA origin to the above knee popliteal artery. Unfortunately, his rest pain worsened.

On exam, he had a femoral pulse only and no distal pulses, only monophonic and weak pedal signals. The right groin wound had been treated for postoperative wound infection and there was still some swelling and a stitch abscess, but no deep infection. CTA showed that his profunda femoral artery had a focal dissection or stenosis at the origin along with overhang of his SFA stents across the origin of the PFA. The SFA stents were occluded along their whole length. There was remnant disease of the external iliac artery as well.

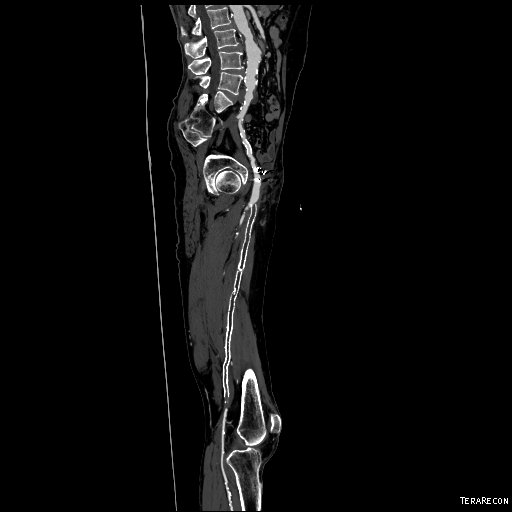
There was reconstitution of a diseased but patent above knee popliteal artery with three vessel runoff. He had had harvest of his greater saphenous vein. Treatment options included multisegment arm vein with redo profundaplasty, but given the inflammation around his recently operated, recently infected groin, I was concerned for wound infection. He was also quite disabled by his worsened pain. The other option was to access the left common femoral artery and placed a sheath up and over and wire across the diseased profunda and intervene on it, but with the stent in place, I would have to place likely another stent across the origin. I could then attempt a bypass with arm vein or prosthetic graft using this compromised artery as inflow for a bypass to the below knee popliteal artery or a tibial vessel but I doubted this would be durable, nor resistant to infection if prosthetic was used.
Remote endarterectomy (EndoRE) gave me a third option. It is a hybrid technique, but based on an old and established technique of open remote endarterectomy dating from the 60’s. Rings (Vollmer Rings, LeMaitre Vascular) are used to dissect occlusive plaque under fluoroscopy, and a cutting ring (Moll Ring Cutter, LeMaitre Vascular) is used to cut the plaque at the chosen location. Because the distal end point of dissection is not surgically exposed, but rather fluoroscopically guided, it is termed Remote Endarterectomy. Wire skills are required to access and repair any dissections that may occur.
I have presented in the past a series of cases where I removed occluded stents. Because the dissection is carried out outside the plaque, it is also outside the stent. Retrograde EndoRE of SFA plaque can be carried out up to the SFA origin, and avoid a groin incision which in this case was important. Therefore, a proximal thigh exposure of the SFA and EndoRE was planned with endovascular access by left CFA as described.
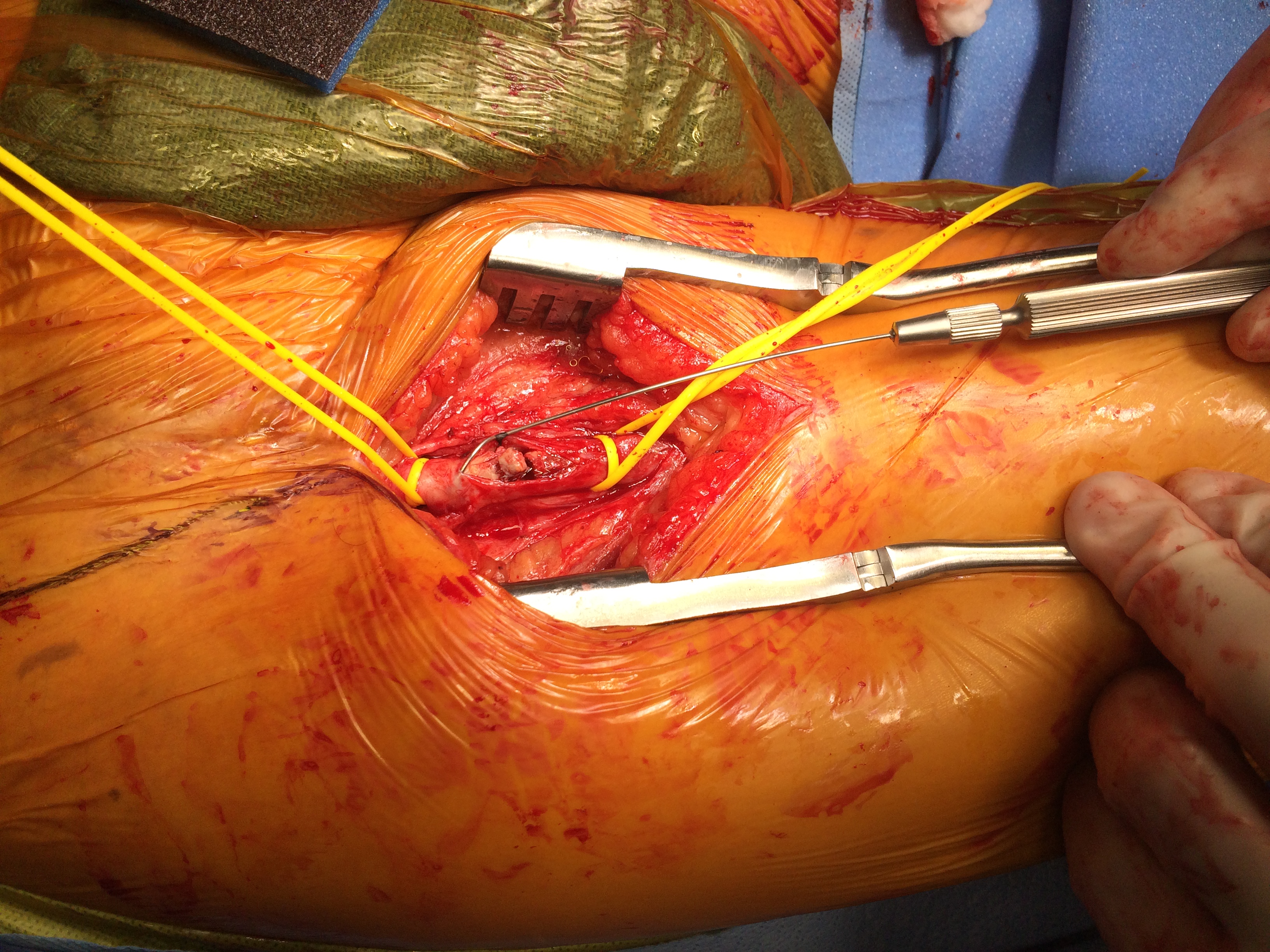
The SFA was a hard, calcified pipe and control was achieved with vessel loops which allow passage of the ring and occlusion of the artery once the plaque and stents were removed. The artery was opened via longitudinal arrteriotomy and the plaque mobilized and divided. The proximal SFA plaque was then dissected (above and below).

There was immediate establishment of a robust pulse in the proximal SFA after removal of the plaque.

Distally, the plaque would not mobilize at a point in the artery where there was laxity in the artery and especially adherent plaque and therefore, the distal SFA was cut down on to reaccess the stent from below.



The arteriotomies were repaired with patch angioplasties using bovine pericardium. This allowed for completing the procedure with endovascular techniques which included the distal end point dissection, profunda stenosis, and external iliac stenosis.



At completion, there was a palpable dorsalis pedis artery pulse. The composite angio with preop CTA centerline reconstruction are shown below.

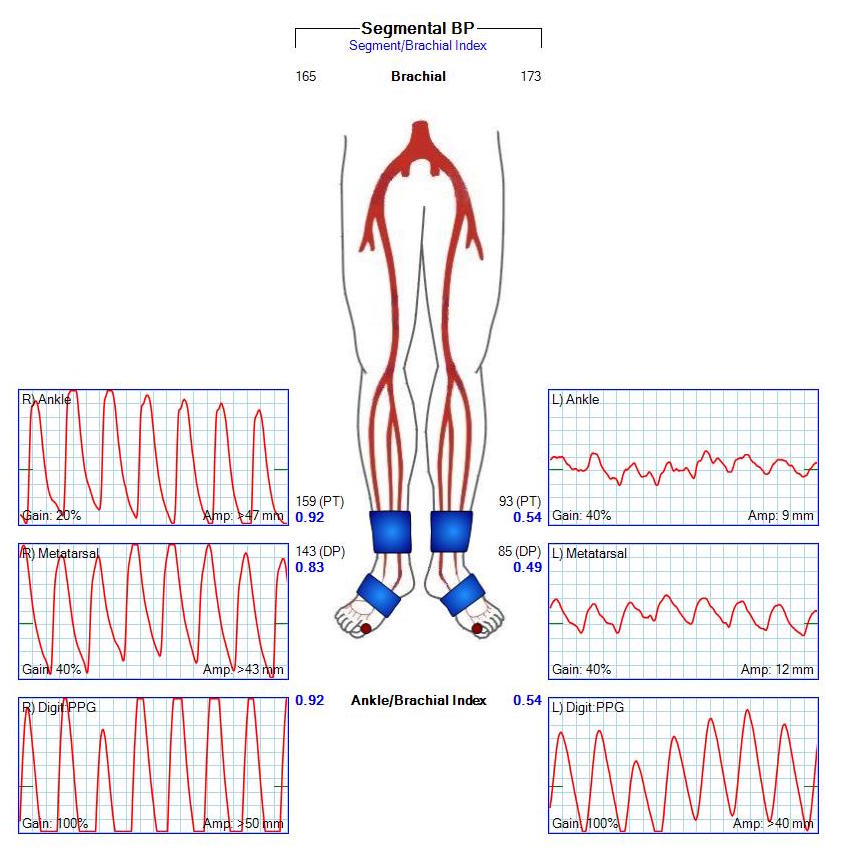
He had relief of his symptoms. Prior to discharge, ABI and PVR’s show normalization of flow to his foot.
Conclusion: In my experience, the longevity of these lesions is dependent on the same factors dictating other revascularizations -excellence of inflow, optimization of profunda outflow, and good tibial outflow. The conduit, being the recanalized original artery, is not as good as a single vein, but it remodels and becomes normal artery based on micro pathology. Failure occurs at the stent with the usual restenosis that can occur in some but not all people, and in isolated points in the artery where likely remnant tissues scar creating focal lesions. Frequent surveillance achieves acceptable primary and secondary patencies. Thromboses do occur. Unlike PTFE grafts, thromboses in EndoRE is usually limited to the recanalized artery without distal embolization. Stent removal is challenging but feasible. In this patient, a second cut down was required to achieve plaque and stent removal. The groin was not re-entered, avoiding dissection in a recently infected, surgical wound. If the popliteal was occluded, a popliteal endarterectomy via a below knee cutdown is possible achieving total femoropopliteal plaque clearance, and the below knee popliteal artery can then be used for a very short bypass to one of the tibial arteries if indicated and if autologous vein is limited in availability.
EndoRE offers a third option after bypass and intervention and should be in a vascular surgeon’s armamentarium.
