

Patient is a younger man who was referred for evaluation of a left common carotid artery aneurysm that complicated Takayasu’s arteritis. He was on maintenance steroids and was asymptomatic, but over a year of surveillance, his aneurysm grew from 2.6 to 2.8cm with encroachment of the aneurysmal segment onto the origin of the LCCA which had a bovine anatomy. Treatment options included continued observation, open repair -direct or extraanatomic, and hybrid endovascular repair.

The patient did not want to undergo sternotomy for definitive repair if less invasive options were available. Considering a subclavian to carotid bypass, the occlusion of the aneurysmal stump would be technically difficult and hazardous for future stroke. Therefore a hybrid repair with exposure of the carotid bifurcation and clamp of the internal carotid artery for cerebral protection was chosen.

In the operating room, the carotid bifurcation was exposed via an oblique skin line incision with the C-arm oriented on the patient’s right. A table was draped off the patient’s left arm which had been prepped for brachial access for aortography. Access was taken from the distal common carotid artery with orientation of the Rosen wire down the descending thoracic aorta -this was to accomodate the nose cone of the device, a Cook 24mm AUI converter with a 12mm iliac extension. This choice of stent grafts accorded with the type of graft I would have chosen for the open repair (Dacron based), and had the appropriate size to exclude the aneurysm from the short proximal neck to the distal segment. The arteries were surrounded by inflammatory tissues and this made dissection challenging but not onerous as a redo dissection.

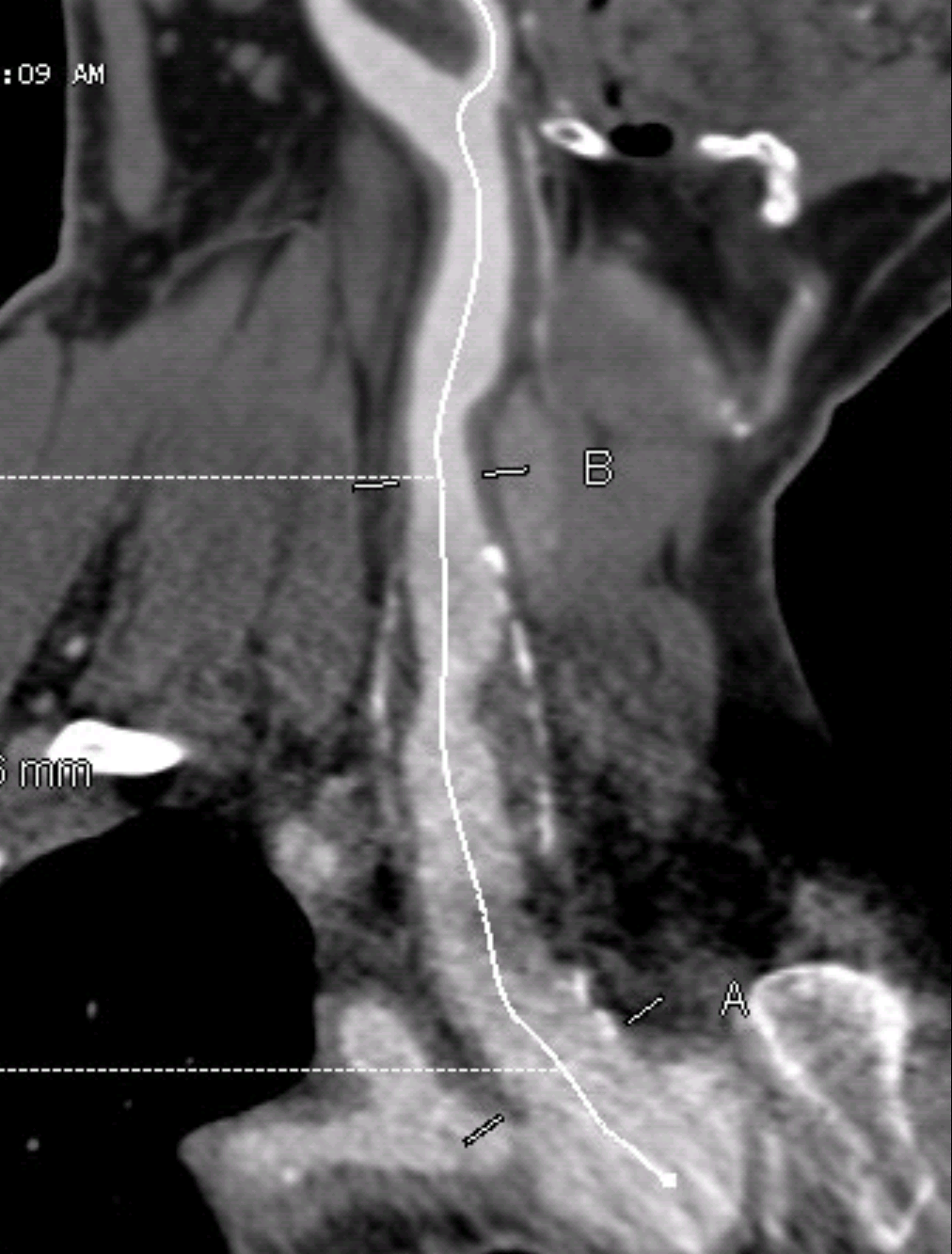
The predeployment arteriogram identified fluoroscopic clues to deployment.

In this patient’s case, the tip of the ET tube provided an excellent reference. (see above composite arteriogram).

Deployment was satisfactory. The arteriotomy, a transverse one I had made to avoid a tear in the thickened, chronically diseased artery, was repaired with running monofilament suture after flushing. The patient did have some oozing because of being on Plavix, but a drain was unnecessary. He awoke neurologically intact and was dimissed on POD#2.

3 replies on “Hybrid endovascular repair of proximal left common carotid artery aneurysm”
Congratulations for the case. A question: why you don’t choose the anterograde way? Thank you
LikeLike
Good question. The stent graft is a Zenith iliac limb which has a short delivery system but correct orientation of tapering size to go from proximal common carotid to distal. The most important consideration is the open exposure allows for cerebral protection by clamping the internal and external carotid arteries. Also the angle is challenging when approached from the femoral access and increases the likelihood of trauma and cerebral embolization.
LikeLike
I’m agreeing with your choose! Thank you
LikeLike