
The proximal anastomosis is the most critical portion of an open aortic aneurysm repair. Several concepts are central to creating an anastomosis that doesn’t bleed at unclamping: managing narrow spaces, overcoming distortion, and using just enough tackle.
Narrow Spaces
The transabdominal exposure is a narrow space. The work is done under the overhanging left renal vein, the transverse colonic mesentery, the liver, the rib cage. Extra lateral space can be made by eviscerating the bowel, but at the cost of higher rates of ileus, and doesn’t solve the first problem. The standard DeBakey aortic clamp and straight Fogarty clamps stand nearly straight up, limiting the space above the incision at the aortic neck. My goto clamp is the Cherry Supra Celiac Aortic Clamp, designed by my mentor Ken Cherry. 
It hugs the contour of the mesentery and liver overhang, and the handles stay out of the way above the wound. It will also tilt up the aorta because of the weight balance. The other option is to apply a transverse clamp, which I will discuss in a later post. The transverse clamp leaves the suprarenal space free of clamp, but can be difficult if not hazardous to apply. The clamp has to be hemostatic and this can be challenging with atherosclerotic plaque -preoperative planning must include planning for safe clamp sites. A suprarenal clamp may be limited by the presence of the terminal insertions of the diaphragmatic crurae. I have recently found that dividing these crurae with a Maryland tipped Ligasure, a laparoscopic instrument I use to dissect the retroperitoneum, makes short order of what can sometimes be an awkward exposure in this tight space. Finally, endarterectomy of the neck should be done carefully to let needles pass without difficulty.
Distortion
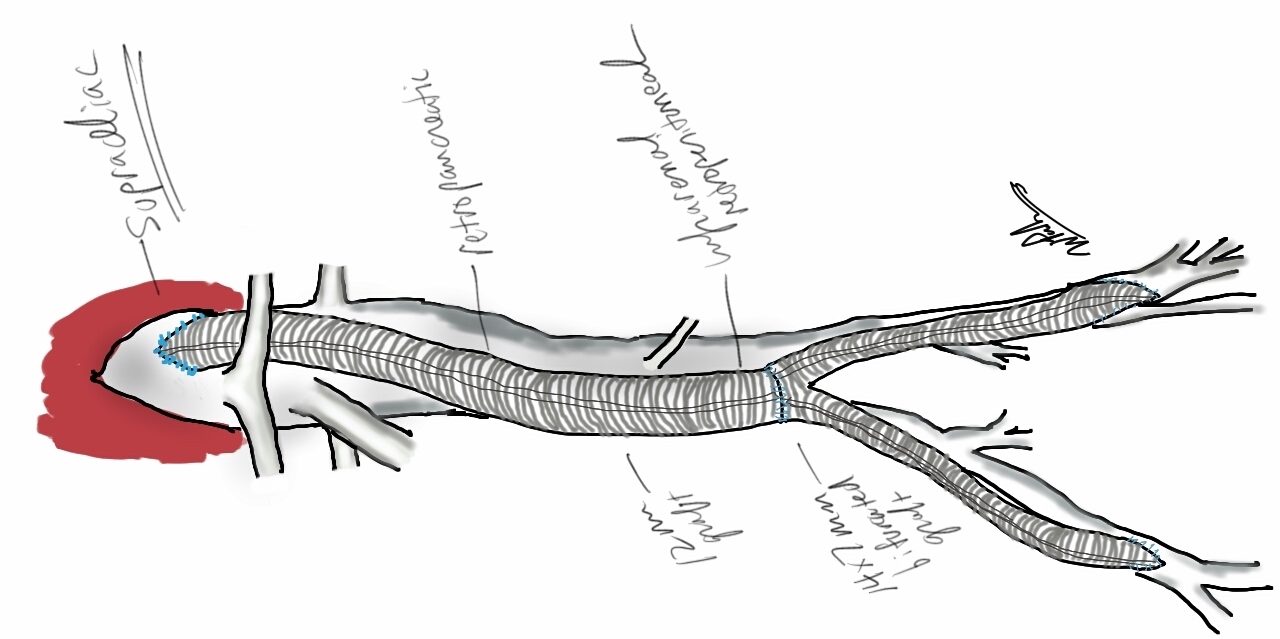
The proximal anastomosis is ideally just another end to end anastomosis -attaching a circle to a circle, but clamping narrows and distorts the circular aortic neck (top illustration). To envision this, imagine the aortic neck being a clock face:

Lets say the suture should be applied at each of the hours and half hours. You get ready to sew your first aortic neck and after endarterectomizing some plaque, you get this:

The important point is that you still have to apply the original plan of applying sutures evenly and at an appropriate frequency (about 3mm apart), to avoid gathers and gaps, especially on the posterior wall. One way is to apply outward tension with a Wheatlander retractor in the aortic sac.

The Right Tackle
You don’t go after panfish with a deep sea tackle. Pictured below are a spinning lure for trolling with a large hook and a small dry fly with narrow guage hook for comparison.

Which hook creates the larger hole in the fish’s mouth? In fact, both lures can be used to catch the same large trout, but in different situations.

Also, because the needles are finer and I favor supersized Castro needle holders. The needle holes which represent rents in the aortic wall are far easier to deal with using a smaller needle. Right tackle.

5 replies on “Avoiding Aortic Exoleaks: principles of the proximal aortic anastomosis”
Should be required reading for trainees (and many in current practice!). The thought underlying the action is the gem.
LikeLike
Good morning. I just watched your home video on laparoscopic aortic repair. I would like to acquire such a set-up, for practice at home. Can you post your email, such that I can email you some questions regarding mirroring your exact set-up?
LikeLike
It’s a wood frame with round eyelets drilled into it. The camera was an Apple video cam although any HD cam that focuses close should work. The grafts are clipped to a flat board. Haven’t used it in years
LikeLike
Good afternoon. Thank you for the reply. Would you be willing to sell me the set-up, if you haven’t used it in years?
Are you using something else?
-CE
LikeLike
[…] of eliminating clamp overhang. Suturing is done with 4-0 Prolene on SH needles -this is plenty (link). The proximal anastomosis wants to bleed, and sewing to a fully cut ring of aorta ensures good […]
LikeLike