

These really are common in the Midwest. When I was a fellow, about one a month was done at the other Clinic. Shamblin, who ironically never went into vascular surgery, wrote the paper with the eponymous classification while a medical student.
October 16, 2008
This patient underwent a screening carotid artery duplex scan, and was found to have a 15mm mass in his carotid bifurcation. He was asymptomatic. On exam, there was a nodule that was palpable through the skin.

He was taken to the operating room with myself and Dr. Simon Wright, otolaryngologist, and we found a small discrete mass basically as anticipated on CT. The incision was along skin lines, and all the nerves were dissected using McCabe clamp. Hemostasis was maintained with sutures, clips, and a harmonic scalpel which was used to avoid transmission of electrical energy into the wound.

The mass gets its perfusion from multiple branches from the external carotid artery. By patiently dissection these, the tumor was dissected and removed. This was a Shamblin Type I lesion (see blog entry). The patient recovered without complication and was discharged the next day.

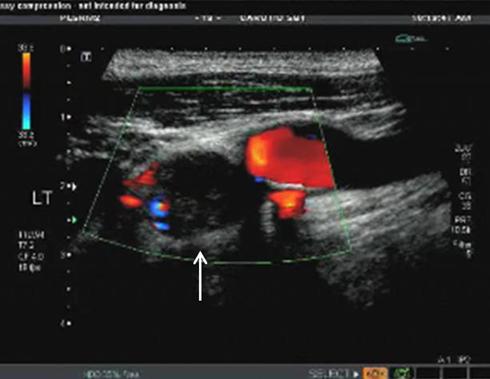
The panel below right shows the screening carotid duplex study which found the lesion. The CTA above shows the lesion in its typical location. The oblique axis MPR view shows the mass to have multiple vascular supply, but to be discrete and not invading the artery. The photos above show the lesion in-situ and ex-vivo.
Path revealed it to be a paraganglionoma.


