
There are several areas yet to be satisfactorily traversed by endovascular technology and the common femoral artery is one area. While not completely a no stent zone, stents and interventions in the CFA do poorly compared to the open surgical alternative. As vascular surgeons we know that the key to inflow problems is the produnda femoris arteria and she does not tolerate being ignored, stented across, or ballooned too much. I have tabulated some areas that are still in the purview of open surgery in no particular order :
1: systemic infection
2: failure of stent grafts
3: rupture/hemorrhage/trauma
4: thoracic outlet obstructions
5: cancer
6: SVC syndrome after failure of interventions
7: MALS
8: popliteal entrapment
9: hypothenar hammer syndrome
10: very large thoracoabdominal or juxtarenal aortic aneurysms (until we get FDA approved off the shelf devices)
11: dialysis access
12: extreme limb salvage
13: severe aortic occlusive disease
14: CKD on the cusp of dialysis
15: congenital vascular disease
17: trauma/contaminated fields
18: low risk patients
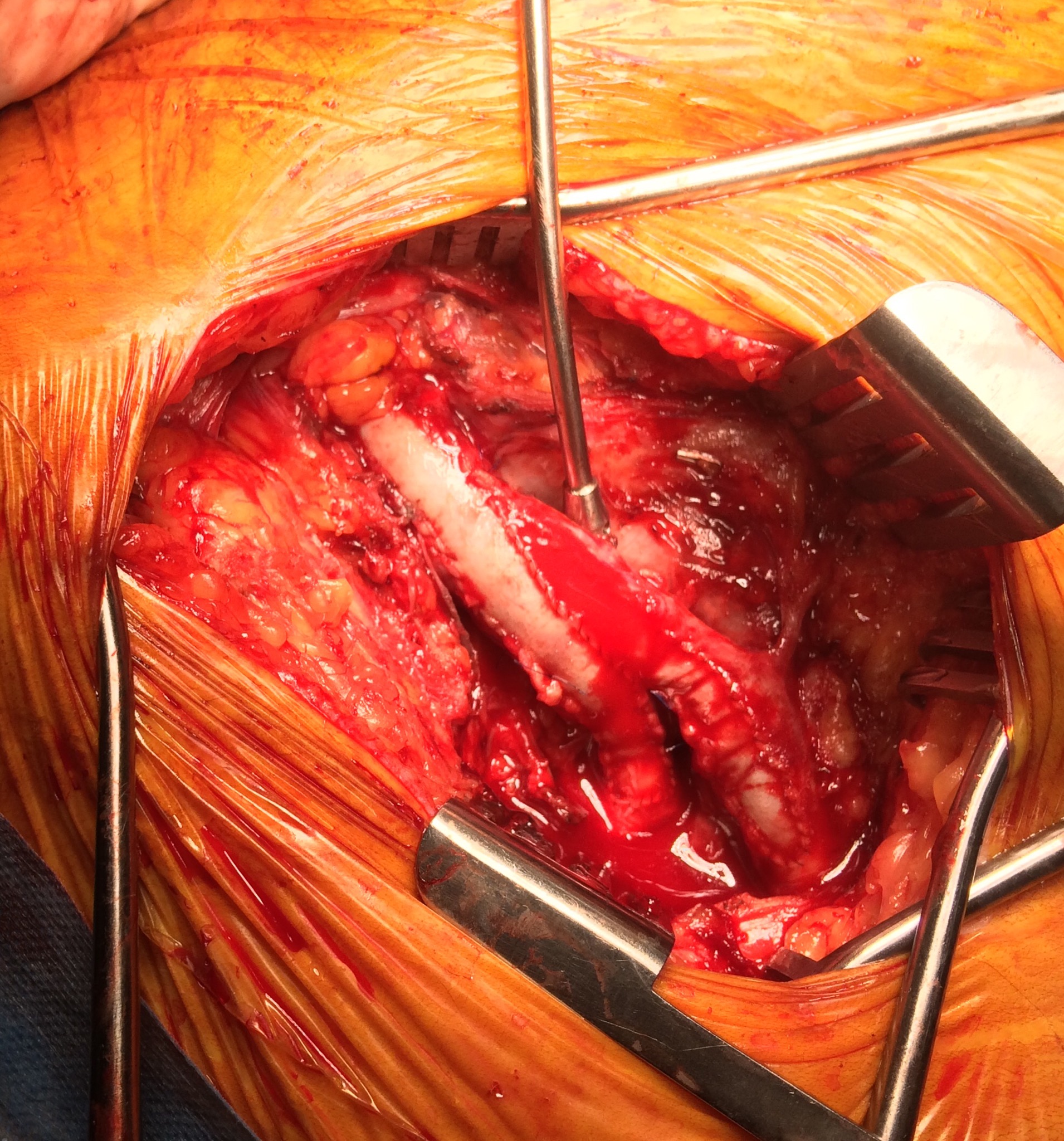
19: common femoral artery
20: subclavian artery/innominate artery
21: carotid endarterectomy -for now
The list is open ended and you may add in the comments below, but the list in some parts is esoteric. The data is sobering if you read “Predicted shortfall in open aneurysm experience for vascular surgery trainees,” by Dua et al in the 10/2014 JVS. When I trained, I graduated with about 50 open AAA under my belt. Dua et al are predicting 10 per trainee in 2015, and 5 per trainee by 2020.
Who will do my open AAA?

