

Type B aortic dissections (TBAD) are frequently seen here at the Clinic as we serve as a regional referral center. As a trainee, I read the chapters discussing all the classifications and discussions of the biomechanics and felt quite intimidated by the all the moving parts involved in an aortic dissection, and I missed the main point about TBAD. Aside from the rupture risk due to the attenuation of the adventitia and hypertension, the acute TBAD is a rapidly developing stenosis of the aorta due to the inflation of a wind sock balloon created by the dissection flap. You can assume any flow that occurs in the false lumen is limited by the area of the proximal tear which is always smaller than the area of the aortic lumen. The true lumen is still perfusing the lower half of the body, and because of the volume filling effect of the flap, flow is restricted. The equivalent physiology is seen in aortic coarctation. Long term, the false lumen behaves like a pseudoaneurysm and may thrombose, continue to grow, or both.
Our group looked at CT’scans on 80 consecutive patients and found that the true lumen to false lumen ratio of less than 0.37 is predictive of the need for intervention.

This makes hemodynamic sense as it approximates the 70% critical stenosis borderline for other arteries. It explains why closing the opening of the dissection, the opening of the wind sock, and expanding the true lumen effectively treats malperfusion.

This patient whose CTA is shown above was transferred with increasing abdominal pain, inability to control blood pressure, and worsening lactic acidosis.

There was nearly complete obliteration of the true lumen throughout the aorta and occlusion of the left renal artery and dissection into the celiac and superior mesenteric arteries.

Aortography showed the dissection, and absence of visceral vessels from the injection which was from the aortic root. True lumen position was confirmed with IVUS.

A thoracic stent graft was delivered across the left subclavian artery origin up to the innominate artery origin -the patient had a bovine arch. Immediately, there was filling of the visceral vessels with re-establishment of true lumen flow.

The renal occlusion appeared improved but there was still a stenosis due to deflated dissection flap and this was stented (panel right above).
His abdominal pain remitted and his lactate normalized. His creatinine stabilized and has since normalized.
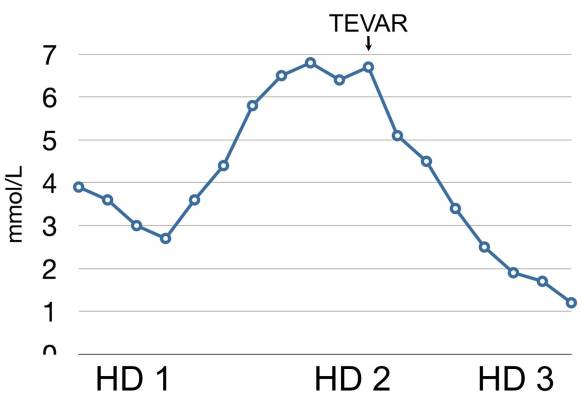
Again, if the true-lumen is compressed, the aorta is stenotic because there is a wind sock inflated in it. TEVAR offers a minimally invasive option, frequently percutaneous, for treating this.
