

When conduit is limited, or PTFE or cadaver vein is being considered, in the setting of occluded SFA stents, I have found that it is possible and perhaps preferable to attempt removal of these stents using remote endarterectomy.



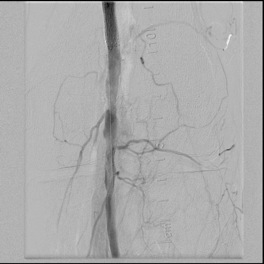
The CTA, particularly with 3D reconstruction, is helpful in planning these cases.
The additional material needed is fluoroscopy and endovascular skills. Directing a subintimal Glidewire helps free the stent and aid passage of the Moll ring dissector.


Adding cold saline seems to help shrink the stents. A plaque free distal end point allow the stents to be removed with a gentle tug.


I put these patients on coumadin anticoagulation. Surveillance is needed for recurrent stenoses -typically these occur randomly as focal TASC A stenoses, and likely represent remnant medial tissues that have caused intimal hyperplasia. This may be particularly amenable to treatment with drug eluting balloons. Failure as thrombosis typically is limited to the treated vessel without the embolism seen when PTFE grafts fail. Failure tends to occur in smokers. Inability to pass the dissector is usually seen in patients with heavy calcification -diabetics, renal failure, and I would avoid attempting remote endarterectomy in these patients. When the dissectors fail to pass, cutting down and directly endarterectomizing the vessel and resuming remote endarterectomy is feasible. The common femoral artery is repaired with a patch. I try to avoid having to place a distal stent and when a tapered end point, as in a successful carotid endarterectomy, is achieved, usually unnecessary.
Parts of this was presented at Midwest Vascular in 2008.
